Venkata S Akshintala, Rishi Subrahmanyan, Anmol Singh, Atif Zaheer, Furqan Bhullar, Ayesha Kamal, Peter J Lee, Maisam A Abu El Haija, Mahya Faghih, Elham Afghani, Vikesh K Singh
{"title":"Discordance Between Radiological and Clinical Findings Among Patients Presenting With Elevated Lipase and Abdominal Pain.","authors":"Venkata S Akshintala, Rishi Subrahmanyan, Anmol Singh, Atif Zaheer, Furqan Bhullar, Ayesha Kamal, Peter J Lee, Maisam A Abu El Haija, Mahya Faghih, Elham Afghani, Vikesh K Singh","doi":"10.14309/ctg.0000000000000861","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>False-positive lipase elevation is a diagnostic challenge in acute pancreatitis (AP) but has not been systematically studied. We evaluated patients presenting with serum lipase elevation and correlated this with abdominal imaging findings, considered the gold standard for AP diagnosis.</p><p><strong>Methods: </strong>Patients with abdominal pain, serum lipase ≥3-fold the upper limit of normal (ULN), and abdominal imaging within 48 hours of their lipase check were identified. An independent expert pancreas radiologist blinded to clinical data reviewed the images for features of AP. For patients without imaging changes of AP, repeat imaging obtained within 30 days was reviewed. Among patients with elevated lipase but no imaging changes of AP, other etiologies of lipase elevation were identified. Patients were stratified by the degree of lipase elevation, and imaging findings were compared between groups.</p><p><strong>Results: </strong>Two hundred thirty-four patients had lipase ≥3-fold the ULN, abdominal pain, and underwent CT or MRI with intravenous contrast. 60.2% had AP findings on their initial imaging, and another 13% had AP or sequelae on imaging within 30 days. In patients without imaging findings of AP, the use of opioid analgesics was the most commonly suspected cause of lipase elevation (24.7%), followed by abdominal trauma/surgery (12.9%). Among lipase elevations, a cutoff of ≥6-fold the ULN had the highest accuracy (70.1%) for diagnosing AP.</p><p><strong>Discussion: </strong>Lipase elevation without imaging findings of AP is found in nearly one-fourth of patients and may suggest non-AP causes of lipase elevation. This has clinical implications, but increasing lipase cutoff to ≥6-fold ULN has only a modest increase in diagnostic accuracy, suggesting the need for a better biomarker for AP diagnosis.</p>","PeriodicalId":10278,"journal":{"name":"Clinical and Translational Gastroenterology","volume":" ","pages":"e00861"},"PeriodicalIF":3.0000,"publicationDate":"2025-06-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12377283/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Translational Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14309/ctg.0000000000000861","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: False-positive lipase elevation is a diagnostic challenge in acute pancreatitis (AP) but has not been systematically studied. We evaluated patients presenting with serum lipase elevation and correlated this with abdominal imaging findings, considered the gold standard for AP diagnosis.
Methods: Patients with abdominal pain, serum lipase ≥3-fold the upper limit of normal (ULN), and abdominal imaging within 48 hours of their lipase check were identified. An independent expert pancreas radiologist blinded to clinical data reviewed the images for features of AP. For patients without imaging changes of AP, repeat imaging obtained within 30 days was reviewed. Among patients with elevated lipase but no imaging changes of AP, other etiologies of lipase elevation were identified. Patients were stratified by the degree of lipase elevation, and imaging findings were compared between groups.
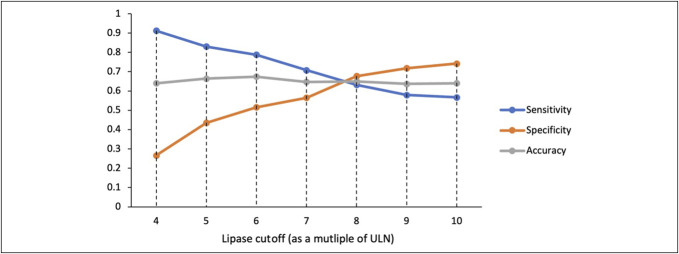
Results: Two hundred thirty-four patients had lipase ≥3-fold the ULN, abdominal pain, and underwent CT or MRI with intravenous contrast. 60.2% had AP findings on their initial imaging, and another 13% had AP or sequelae on imaging within 30 days. In patients without imaging findings of AP, the use of opioid analgesics was the most commonly suspected cause of lipase elevation (24.7%), followed by abdominal trauma/surgery (12.9%). Among lipase elevations, a cutoff of ≥6-fold the ULN had the highest accuracy (70.1%) for diagnosing AP.
Discussion: Lipase elevation without imaging findings of AP is found in nearly one-fourth of patients and may suggest non-AP causes of lipase elevation. This has clinical implications, but increasing lipase cutoff to ≥6-fold ULN has only a modest increase in diagnostic accuracy, suggesting the need for a better biomarker for AP diagnosis.
期刊介绍:
Clinical and Translational Gastroenterology (CTG), published on behalf of the American College of Gastroenterology (ACG), is a peer-reviewed open access online journal dedicated to innovative clinical work in the field of gastroenterology and hepatology. CTG hopes to fulfill an unmet need for clinicians and scientists by welcoming novel cohort studies, early-phase clinical trials, qualitative and quantitative epidemiologic research, hypothesis-generating research, studies of novel mechanisms and methodologies including public health interventions, and integration of approaches across organs and disciplines. CTG also welcomes hypothesis-generating small studies, methods papers, and translational research with clear applications to human physiology or disease.
Colon and small bowel
Endoscopy and novel diagnostics
Esophagus
Functional GI disorders
Immunology of the GI tract
Microbiology of the GI tract
Inflammatory bowel disease
Pancreas and biliary tract
Liver
Pathology
Pediatrics
Preventative medicine
Nutrition/obesity
Stomach.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


