Objectively measured activity behaviours using the ActivPAL accelerometer following robotic and manually performed total knee arthroplasty : a feasibility study from a randomized controlled trial (ROAM study).
Nick D Clement, Bola Ajekigbe, Jayasree Ramaskandhan, Steven Galloway, Karen Smith, David J Weir, David J Deehan
{"title":"Objectively measured activity behaviours using the ActivPAL accelerometer following robotic and manually performed total knee arthroplasty : a feasibility study from a randomized controlled trial (ROAM study).","authors":"Nick D Clement, Bola Ajekigbe, Jayasree Ramaskandhan, Steven Galloway, Karen Smith, David J Weir, David J Deehan","doi":"10.1302/2046-3758.146.BJR-2024-0239.R1","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>To assess whether it was feasible to objectively measure activity behaviour between robotic arm-assisted (raTKA) and manually performed (mTKA) total knee arthroplasty using the ActivPAL accelerometer.</p><p><strong>Methods: </strong>A randomized controlled trial was undertaken and a subgroup of 40 patients underwent physical activity assessment. Patients were randomized to either mTKA (n = 18) or raTKA (n = 22). Preoperative (baseline) and 12-month postoperative physical activity assessment were undertaken using the ActivPAL accelerometer in addition to patient-reported outcome measures (PROMs): Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Forgotten Joint Score (FJS), EuroQol five-dimension questionnaire (EQ-5D), and EuroQol visual analogue scale (EQ-VAS). At 12 months, 15 patients in the raTKA group and nine in the mTKA group had paired ActivPAL data for analysis. Of the 16 patients without data, four withdrew, four were not provided with the ActivPAL due to logistical reasons, one failed to return the ActivPAL, one was allergic to the ActivPAL patch, and six failed to record or the data were corrupt.</p><p><strong>Results: </strong>There were no significant differences in the improvement in standing time (mean difference (MD) 1.6, p = 0.924), step number (MD 62.0, p = 0.970), sitting time (16.3, p = 0.777), number of sit-to-stand transitions (MD 16.3, p = 0.579), or activity scores (MD 0.0, p = 0.977) between the groups. However, the raTKA had a clinically meaningful and significantly (MD 19.8, 95% CI 0.8 to 38.8; p = 0.041) greater improvement in knee-specific pain according to the WOMAC pain score. There were no other statistically significant (p ≥ 0.113) differences between the other PROMs. There were no significant (p ≥ 0.144) correlations between changes in measures of physical activity functional assessments.</p><p><strong>Conclusion: </strong>Objectively assessed physical activity was logistically difficult due to patient and data loss. There were no differences in activity with small effect sizes (≤ 0.2) between the raTKA and mTKA groups, despite differences in subjective knee pain. Improvement in subjective PROMs did not correlate with objectively measured physical activity, and the two seemed to be independent of one another.</p>","PeriodicalId":9074,"journal":{"name":"Bone & Joint Research","volume":"14 6","pages":"495-505"},"PeriodicalIF":5.1000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12126250/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bone & Joint Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1302/2046-3758.146.BJR-2024-0239.R1","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CELL & TISSUE ENGINEERING","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: To assess whether it was feasible to objectively measure activity behaviour between robotic arm-assisted (raTKA) and manually performed (mTKA) total knee arthroplasty using the ActivPAL accelerometer.
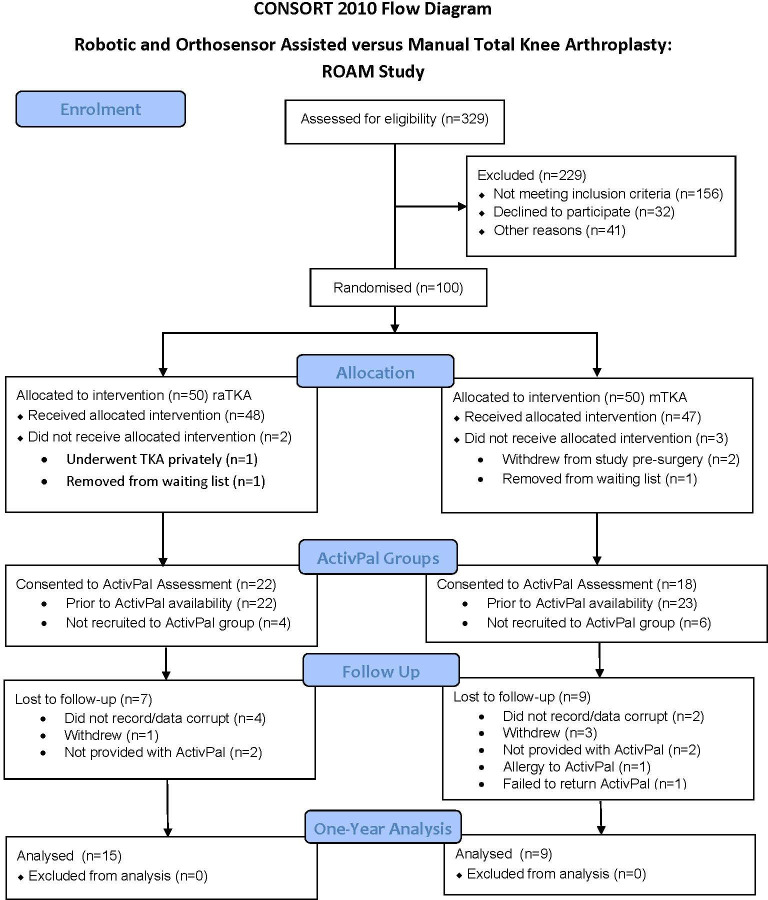
Methods: A randomized controlled trial was undertaken and a subgroup of 40 patients underwent physical activity assessment. Patients were randomized to either mTKA (n = 18) or raTKA (n = 22). Preoperative (baseline) and 12-month postoperative physical activity assessment were undertaken using the ActivPAL accelerometer in addition to patient-reported outcome measures (PROMs): Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Forgotten Joint Score (FJS), EuroQol five-dimension questionnaire (EQ-5D), and EuroQol visual analogue scale (EQ-VAS). At 12 months, 15 patients in the raTKA group and nine in the mTKA group had paired ActivPAL data for analysis. Of the 16 patients without data, four withdrew, four were not provided with the ActivPAL due to logistical reasons, one failed to return the ActivPAL, one was allergic to the ActivPAL patch, and six failed to record or the data were corrupt.
Results: There were no significant differences in the improvement in standing time (mean difference (MD) 1.6, p = 0.924), step number (MD 62.0, p = 0.970), sitting time (16.3, p = 0.777), number of sit-to-stand transitions (MD 16.3, p = 0.579), or activity scores (MD 0.0, p = 0.977) between the groups. However, the raTKA had a clinically meaningful and significantly (MD 19.8, 95% CI 0.8 to 38.8; p = 0.041) greater improvement in knee-specific pain according to the WOMAC pain score. There were no other statistically significant (p ≥ 0.113) differences between the other PROMs. There were no significant (p ≥ 0.144) correlations between changes in measures of physical activity functional assessments.
Conclusion: Objectively assessed physical activity was logistically difficult due to patient and data loss. There were no differences in activity with small effect sizes (≤ 0.2) between the raTKA and mTKA groups, despite differences in subjective knee pain. Improvement in subjective PROMs did not correlate with objectively measured physical activity, and the two seemed to be independent of one another.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


