Nicole F O'Brien, Taty Tshimanga, Florette Yumsa Mangwangu, Ludovic Mayindombe, Robert Tandjeka Ekandji, Jean Pongo Mbaka, Tusekile Phiri, Sylvester June, Montfort Bernard Gushu, Hunter Wynkoop, Marlina Lovett
{"title":"The brain shock index: repurposing the Lindegaard ratio for detecting cerebral hypoperfusion in children with cerebral malaria.","authors":"Nicole F O'Brien, Taty Tshimanga, Florette Yumsa Mangwangu, Ludovic Mayindombe, Robert Tandjeka Ekandji, Jean Pongo Mbaka, Tusekile Phiri, Sylvester June, Montfort Bernard Gushu, Hunter Wynkoop, Marlina Lovett","doi":"10.1186/s13089-025-00430-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Transcranial doppler ultrasound (TCD) allows for the assessment of the cerebrovascular hemodynamics in critically ill children. Given the increasing availability of machines equipped with TCD capabilities globally, it may be a useful approach to detect cerebral hypoperfusion and guide neurologic resuscitation for pediatric patients in resource limited settings where other neuromonitoring techniques are unavailable. However, the current need to evaluate waveform characteristics and to age correct values to determine if a study is abnormal decreases the feasibility of using point of care TCD in this way. The brain shock index (BSI), a repurposing of the Lindegaard Ratio, overcomes these limitations.</p><p><strong>Methods: </strong>We performed a prospective study of children with cerebral malaria (CM). On admission and daily thereafter, TCD was used to evaluate the middle cerebral (MCA) and extra-cranial carotid arteries (Ex-ICA), and the BSI was calculated bilaterally (MCA mean flow velocity ((Vm))/Ex-ICA Vm). Neurologic outcome at discharge was assessed.</p><p><strong>Results: </strong>A cohort of 291 children with CM were evaluated. BSI calculation was successful in all of them. The mean time to perform TCD and calculate the BSI was 4 ± 2 min. Overall, 222 participants (76%) had a good outcome and 69 (24%) a poor outcome. The BSI had an AUC of 0.98 (95% CI 0.97-0.99, p < 0.0001) to predict death or moderate to severe disability. The highest sensitivity and specificity of the BSI to predict adverse outcomes occurred at a cut off value ≤ 1.1. The adjusted odds ratio of poor outcome was 3.2 (95% CI 1.6-6.1, p = 0.001) if any BSI measurement during hospitalization fell below this threshold. No intracranial pressure monitoring was available to determine the relationship between the BSIs and an invasively measured cerebral perfusion pressure.</p><p><strong>Conclusion: </strong>The BSI is a rapid, feasible point of care ultrasound measurement of cerebral hypoperfusion, with values ≤ 1.1 strongly correlating with poor neurologic outcomes in children with CM. Future studies should be performed to assess the utility of BSI to detect the presence and measure the severity of reduced cerebral perfusion pressure in other populations of critically ill children.</p>","PeriodicalId":36911,"journal":{"name":"Ultrasound Journal","volume":"17 1","pages":"27"},"PeriodicalIF":2.9000,"publicationDate":"2025-05-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12125453/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-025-00430-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Transcranial doppler ultrasound (TCD) allows for the assessment of the cerebrovascular hemodynamics in critically ill children. Given the increasing availability of machines equipped with TCD capabilities globally, it may be a useful approach to detect cerebral hypoperfusion and guide neurologic resuscitation for pediatric patients in resource limited settings where other neuromonitoring techniques are unavailable. However, the current need to evaluate waveform characteristics and to age correct values to determine if a study is abnormal decreases the feasibility of using point of care TCD in this way. The brain shock index (BSI), a repurposing of the Lindegaard Ratio, overcomes these limitations.
Methods: We performed a prospective study of children with cerebral malaria (CM). On admission and daily thereafter, TCD was used to evaluate the middle cerebral (MCA) and extra-cranial carotid arteries (Ex-ICA), and the BSI was calculated bilaterally (MCA mean flow velocity ((Vm))/Ex-ICA Vm). Neurologic outcome at discharge was assessed.
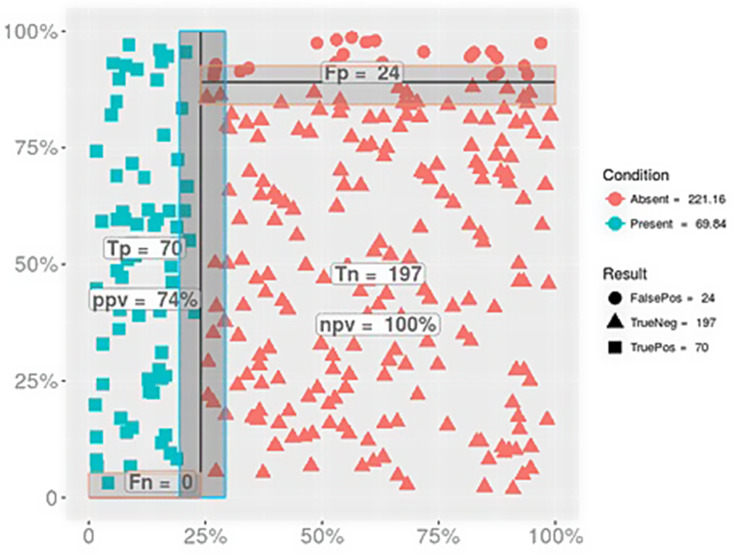
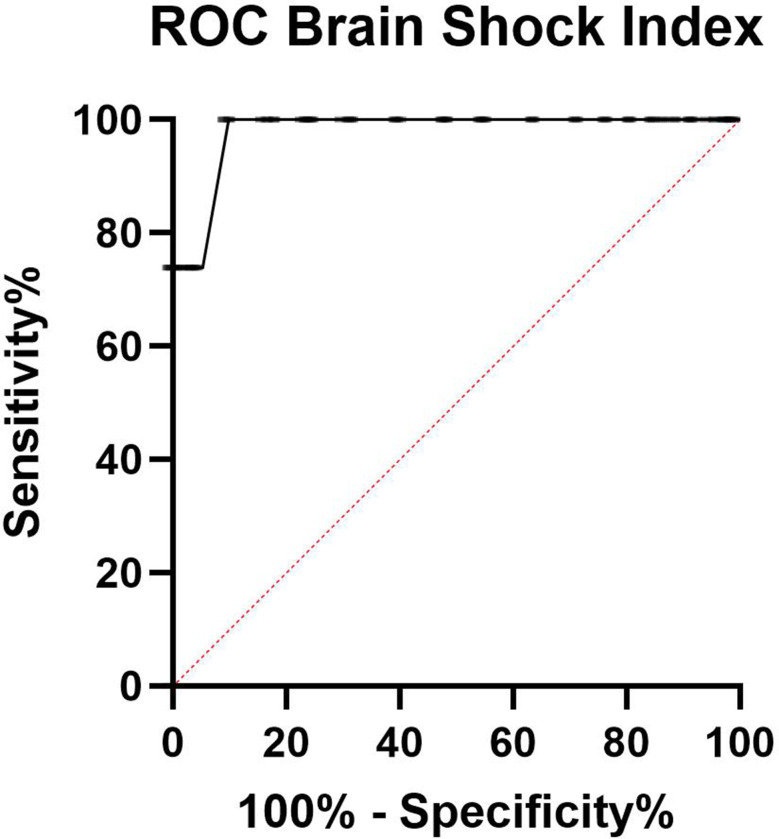
Results: A cohort of 291 children with CM were evaluated. BSI calculation was successful in all of them. The mean time to perform TCD and calculate the BSI was 4 ± 2 min. Overall, 222 participants (76%) had a good outcome and 69 (24%) a poor outcome. The BSI had an AUC of 0.98 (95% CI 0.97-0.99, p < 0.0001) to predict death or moderate to severe disability. The highest sensitivity and specificity of the BSI to predict adverse outcomes occurred at a cut off value ≤ 1.1. The adjusted odds ratio of poor outcome was 3.2 (95% CI 1.6-6.1, p = 0.001) if any BSI measurement during hospitalization fell below this threshold. No intracranial pressure monitoring was available to determine the relationship between the BSIs and an invasively measured cerebral perfusion pressure.
Conclusion: The BSI is a rapid, feasible point of care ultrasound measurement of cerebral hypoperfusion, with values ≤ 1.1 strongly correlating with poor neurologic outcomes in children with CM. Future studies should be performed to assess the utility of BSI to detect the presence and measure the severity of reduced cerebral perfusion pressure in other populations of critically ill children.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


