Kenan Kherallah, Imran Ahmad, Anishka Bandara, Jacob Kattoula, Ivan Rodriguez, Scott Worswick
{"title":"Adverse Cutaneous Reactions to Monoclonal Antibodies: Stevens-Johnson Syndrome, Toxic Epidermal Necrolysis, Erythema Multiforme, and Fixed Drug Eruption - A Systematic Review.","authors":"Kenan Kherallah, Imran Ahmad, Anishka Bandara, Jacob Kattoula, Ivan Rodriguez, Scott Worswick","doi":"10.1159/000545623","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The therapeutic use of monoclonal antibodies (mAbs) has significantly increased since the first mAb was introduced. Despite their therapeutic benefits, mAbs have been accompanied by a rise in adverse effects, affecting various organ systems including the skin. This systematic review consolidates the current literature on the incidence, characteristics, and management of adverse dermatological events (ADEs) post-mAb treatment, focusing on Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), erythema multiforme (EM), and fixed drug eruption (FDE).</p><p><strong>Methods: </strong>A comprehensive PubMed search from 1980 to January 2024 included studies on mAbs causing SJS, TEN, EM, or FDE in humans. Screening was conducted using Covidence, and data were extracted on demographics, mAb details, rash characteristics, and treatment.</p><p><strong>Results: </strong>Of the initial 2002 articles, 29 met the inclusion criteria, highlighting 31 cases of ADEs. The onset of these rashes was delayed, often occurring significantly after starting mAb therapy, with a mean onset time considerably longer than that associated with traditional drugs. Additionally, neither patient sex nor concurrent medication use affected the likelihood of developing these reactions.</p><p><strong>Conclusion: </strong>This review underscores the prolonged timeline for the onset of ADEs from mAbs, distinct from reactions induced by traditional drugs, aligning with the characteristics of progressive immunotherapy-related mucocutaneous eruption. The lack of correlation with patient sex or concurrent medications reaffirms the inherent risk of mAbs. These findings highlight the need for clinicians to monitor and educate patients about the potential for delayed dermatological reactions from mAb treatment to ensure timely management and better outcomes.</p>","PeriodicalId":101351,"journal":{"name":"Biomedicine hub","volume":"10 1","pages":"105-115"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12121980/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biomedicine hub","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000545623","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The therapeutic use of monoclonal antibodies (mAbs) has significantly increased since the first mAb was introduced. Despite their therapeutic benefits, mAbs have been accompanied by a rise in adverse effects, affecting various organ systems including the skin. This systematic review consolidates the current literature on the incidence, characteristics, and management of adverse dermatological events (ADEs) post-mAb treatment, focusing on Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), erythema multiforme (EM), and fixed drug eruption (FDE).
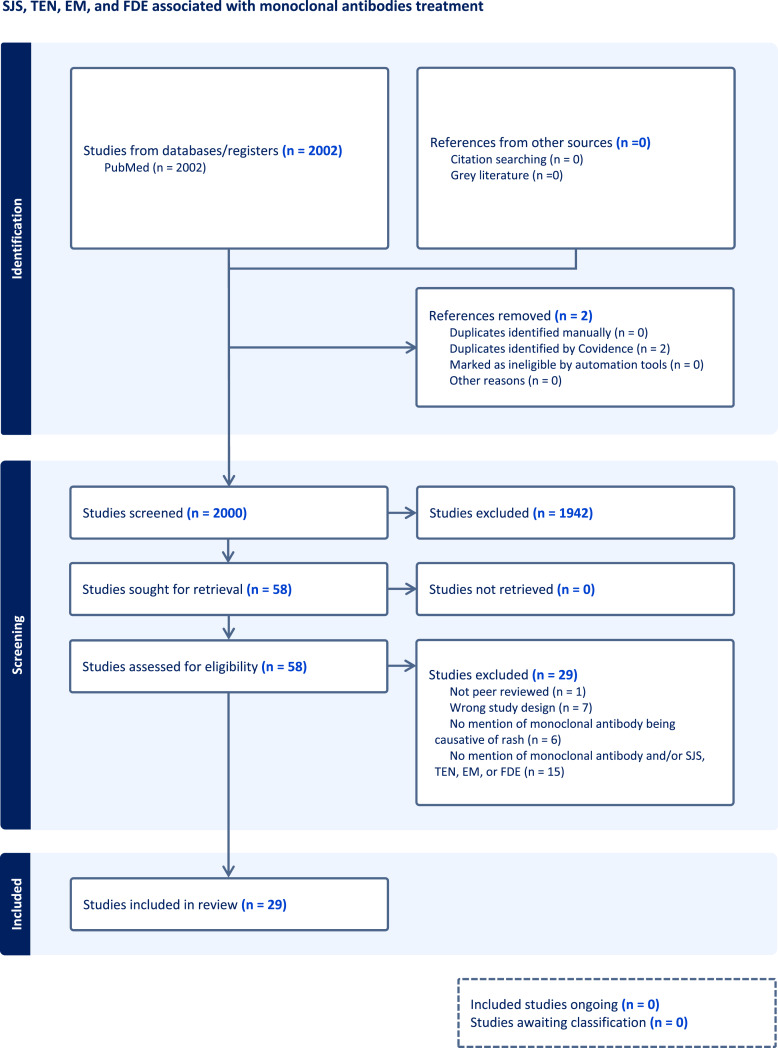
Methods: A comprehensive PubMed search from 1980 to January 2024 included studies on mAbs causing SJS, TEN, EM, or FDE in humans. Screening was conducted using Covidence, and data were extracted on demographics, mAb details, rash characteristics, and treatment.
Results: Of the initial 2002 articles, 29 met the inclusion criteria, highlighting 31 cases of ADEs. The onset of these rashes was delayed, often occurring significantly after starting mAb therapy, with a mean onset time considerably longer than that associated with traditional drugs. Additionally, neither patient sex nor concurrent medication use affected the likelihood of developing these reactions.
Conclusion: This review underscores the prolonged timeline for the onset of ADEs from mAbs, distinct from reactions induced by traditional drugs, aligning with the characteristics of progressive immunotherapy-related mucocutaneous eruption. The lack of correlation with patient sex or concurrent medications reaffirms the inherent risk of mAbs. These findings highlight the need for clinicians to monitor and educate patients about the potential for delayed dermatological reactions from mAb treatment to ensure timely management and better outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


