Mohammad Z Khrais, Jake Smith, Tanmay Gandhi, Shahrukh Arif, Juan Carlos Rico
{"title":"A cautionary tale of false-positive histoplasma urine antigen in an HIV patient: a case report.","authors":"Mohammad Z Khrais, Jake Smith, Tanmay Gandhi, Shahrukh Arif, Juan Carlos Rico","doi":"10.1099/acmi.0.000929.v3","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction.</b> Coccidioidomycosis, or Valley fever, is a fungal disease caused by <i>Coccidioides</i> species, prevalent in parts of the southwestern United States. It usually results from inhaling spores from soil and is a common cause of pneumonia in these regions. <b>Case Presentation.</b> We present a unique case of coccidioidomycosis in an immunodeficient male patient secondary to human immunodeficiency virus infection with poor adherence to anti-retroviral treatment. After presenting with non-specific symptoms and pre-syncope, he was initially diagnosed with pneumonia based on chest X-ray findings, but his symptoms failed to improve with antibiotics. He was treated for presumed pulmonary histoplasmosis following a positive histoplasma urine antigen test. However, the patient worsened clinically. Following a computed tomography scan demonstrating a large necrotic lung consolidation, fungal stain and culture of tissue biopsied through endobronchial ultrasound confirmed coccidioidomycosis. The patient received 2 weeks of liposomal amphotericin with clinical improvement before discharge with itraconazole. <b>Conclusion.</b> The histoplasma antigen test can be falsely positive due to cross-reaction with other fungal infections like blastomycosis, paracoccidioidomycosis or talaromycosis, and less frequently, coccidioidomycosis or aspergillosis. Diagnosis of coccidioidomycosis requires a high index of suspicion outside the expected geographic distribution in the appropriate clinical setting. Our case highlights the risk of false-positive antigen test results and the importance of invasive diagnostics, including bronchoscopy to obtain fungal cultures, if the diagnosis remains uncertain.</p>","PeriodicalId":94366,"journal":{"name":"Access microbiology","volume":"7 5","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-05-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12120142/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Access microbiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1099/acmi.0.000929.v3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
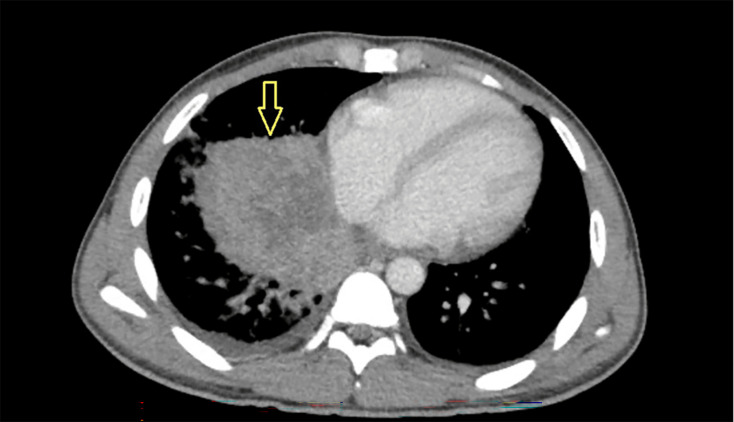
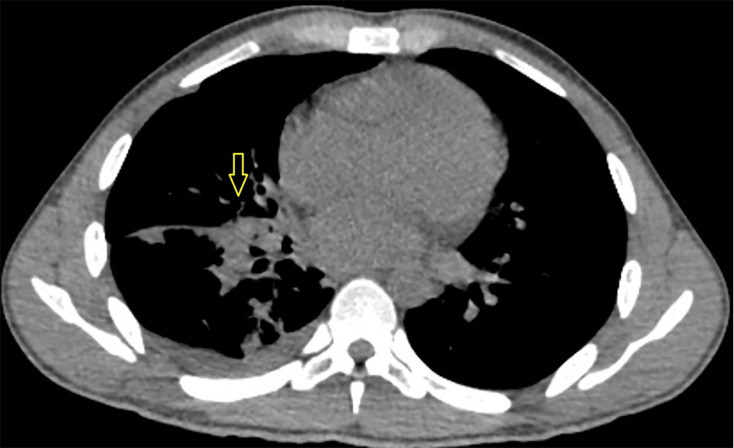
Introduction. Coccidioidomycosis, or Valley fever, is a fungal disease caused by Coccidioides species, prevalent in parts of the southwestern United States. It usually results from inhaling spores from soil and is a common cause of pneumonia in these regions. Case Presentation. We present a unique case of coccidioidomycosis in an immunodeficient male patient secondary to human immunodeficiency virus infection with poor adherence to anti-retroviral treatment. After presenting with non-specific symptoms and pre-syncope, he was initially diagnosed with pneumonia based on chest X-ray findings, but his symptoms failed to improve with antibiotics. He was treated for presumed pulmonary histoplasmosis following a positive histoplasma urine antigen test. However, the patient worsened clinically. Following a computed tomography scan demonstrating a large necrotic lung consolidation, fungal stain and culture of tissue biopsied through endobronchial ultrasound confirmed coccidioidomycosis. The patient received 2 weeks of liposomal amphotericin with clinical improvement before discharge with itraconazole. Conclusion. The histoplasma antigen test can be falsely positive due to cross-reaction with other fungal infections like blastomycosis, paracoccidioidomycosis or talaromycosis, and less frequently, coccidioidomycosis or aspergillosis. Diagnosis of coccidioidomycosis requires a high index of suspicion outside the expected geographic distribution in the appropriate clinical setting. Our case highlights the risk of false-positive antigen test results and the importance of invasive diagnostics, including bronchoscopy to obtain fungal cultures, if the diagnosis remains uncertain.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


