Andreas Martin Studer, Jörg Krebs, Christine Brambs, Corina Christmann-Schmid
{"title":"The Learning Curve for Laparoscopic Sacrocolpopexy Based on Dissection Skills if Structured Teaching and Standardized Surgery are Applied.","authors":"Andreas Martin Studer, Jörg Krebs, Christine Brambs, Corina Christmann-Schmid","doi":"10.2147/AMEP.S513699","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Teaching is an important but time- and resource-consuming process. Therefore, it is important to optimize and structure it effectively. The aim of this study was to evaluate if dry-lab suture and knotting training lead to stable theater performance. Consequently, the learning curve is supposed to be ascribed to only on-patient trainable skills like tissue preparation.</p><p><strong>Patients and methods: </strong>To test this hypothesis, a structured training and stepwise surgical program were implemented to perform laparoscopic sacrocolpopexy (SCP) for urogynecological fellows adapting existing literature.The program was structured and recorded as following: dry-lab training weekly for knotting and suturing skills, assisting 20 SCP, stepwise overtaking defined steps under supervision including preparation of the dissecting planes anteriorly, posteriorly and at the level of the promontory, mesh fixation and retroperitoneal closure. All women opting for sacrocolpopexy as pelvic organ prolapse repair and being treated by one designated fellow were included without any specific selection. The only exclusion criterium was repeat sacrocolpopexy.</p><p><strong>Results: </strong>Within 45 procedures, the fellow reached a plateau of 80 minutes surgical time for SCP (excluding port-entry/-closure or concomitant interventions like hysterectomy or adnexectomy), with a complication rate of 11.1%. A high subjective and objective success rate was reported post-operatively. Differences in overall time were clearly correlated with overall dissection time.</p><p><strong>Conclusion: </strong>We demonstrated that a stepwise, structured, and standardized intraoperative surgical program facilitated safe and efficient laparoscopic SCP performance in the analyzed situation. Off-patient trainable skills like suturing and knotting led to consistent mesh fixation times from the start of the qualification process and variation arose due to in situ learnable factors.</p>","PeriodicalId":47404,"journal":{"name":"Advances in Medical Education and Practice","volume":"16 ","pages":"917-925"},"PeriodicalIF":1.7000,"publicationDate":"2025-05-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12118485/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Medical Education and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/AMEP.S513699","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"EDUCATION, SCIENTIFIC DISCIPLINES","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Teaching is an important but time- and resource-consuming process. Therefore, it is important to optimize and structure it effectively. The aim of this study was to evaluate if dry-lab suture and knotting training lead to stable theater performance. Consequently, the learning curve is supposed to be ascribed to only on-patient trainable skills like tissue preparation.
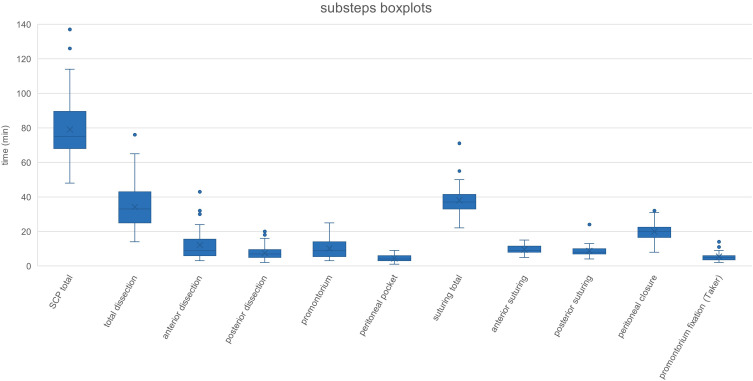
Patients and methods: To test this hypothesis, a structured training and stepwise surgical program were implemented to perform laparoscopic sacrocolpopexy (SCP) for urogynecological fellows adapting existing literature.The program was structured and recorded as following: dry-lab training weekly for knotting and suturing skills, assisting 20 SCP, stepwise overtaking defined steps under supervision including preparation of the dissecting planes anteriorly, posteriorly and at the level of the promontory, mesh fixation and retroperitoneal closure. All women opting for sacrocolpopexy as pelvic organ prolapse repair and being treated by one designated fellow were included without any specific selection. The only exclusion criterium was repeat sacrocolpopexy.
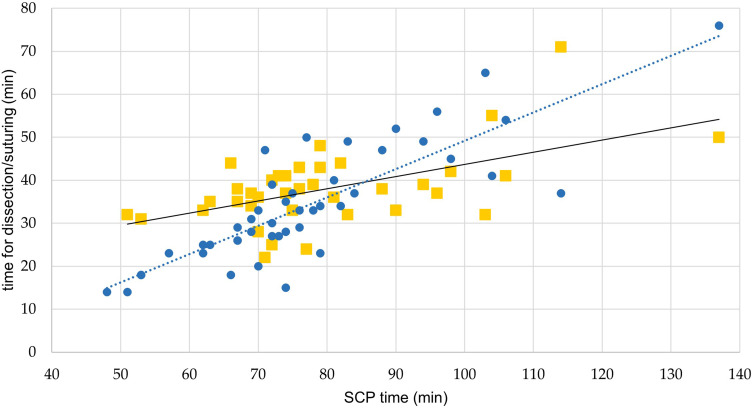
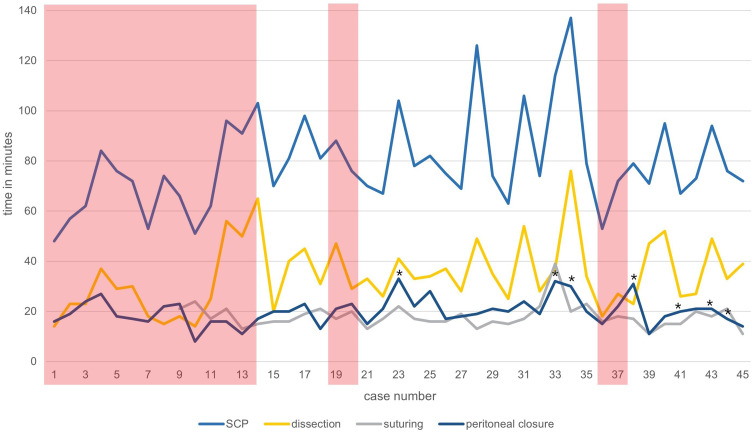
Results: Within 45 procedures, the fellow reached a plateau of 80 minutes surgical time for SCP (excluding port-entry/-closure or concomitant interventions like hysterectomy or adnexectomy), with a complication rate of 11.1%. A high subjective and objective success rate was reported post-operatively. Differences in overall time were clearly correlated with overall dissection time.
Conclusion: We demonstrated that a stepwise, structured, and standardized intraoperative surgical program facilitated safe and efficient laparoscopic SCP performance in the analyzed situation. Off-patient trainable skills like suturing and knotting led to consistent mesh fixation times from the start of the qualification process and variation arose due to in situ learnable factors.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


