María Tamargo, Enrique Gutiérrez, Jorge García Carreño, María Eugenia Vázquez Álvarez, Ricardo Sanz-Ruiz, Mike Huanca, Erika Ludeña, Javier Soriano, Jaime Elízaga, Francisco Fernández-Avilés, Javier Bermejo
{"title":"[[Projection selection and rapid atrial pacing improves early outcomes after self-expanding transcatheter aortic valves]].","authors":"María Tamargo, Enrique Gutiérrez, Jorge García Carreño, María Eugenia Vázquez Álvarez, Ricardo Sanz-Ruiz, Mike Huanca, Erika Ludeña, Javier Soriano, Jaime Elízaga, Francisco Fernández-Avilés, Javier Bermejo","doi":"10.24875/RECIC.M24000497","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction and objectives: </strong>Because of the potential need for permanent pacemaker implantation, patients are frequently monitored for days after transcatheter aortic valve implantation (TAVI), particularly when using self-expanding valves. We sought to determine whether the appearance and management of conduction disturbances after TAVI can be improved by combining the cusp overlap projection (COP) and a rapid atrial pacing (RAP) protocol to detect the need for pacemaker implantation.</p><p><strong>Methods: </strong>We consecutively studied a total of 273 patients who underwent TAVI with self-expanding valves from 2018 through 2022 (134 undergoing standard implantations and 139 COP + RAP). Assessment included the 90-day follow-up.</p><p><strong>Results: </strong>Complete heart block was reported in 25.4% and 14.4% in the standard-of-care and COP + RAP group, with a marked decrease in transient atrioventricular block (12.8% vs 2.9%, respectively; <i>P</i> = .007). The absence of the Wenckebach phenomenon during RAP had a negative predictive value of 97% (95%CI, 91-99) for pacemaker implantation at the follow-up, which significantly decreased the need for 24-hour temporary pacemaker monitoring in the COP + RAP group (91.8% vs 28.1%; <i>P</i> < .0001) and the median [IQR] length of stay (5.0 [4-8] days vs 2.0 [1-4] days; <i>P</i> < .0001). At the 90-day follow-up, COP + RAP reduced pacemaker implantation (OR, 0.48; 95%CI, 0.24-0.92; <i>P</i> = .031), as well as the risk of infection-related readmissions significantly (OR, 0.35; 95%CI, 0.12-0.89; <i>P</i> = .036).</p><p><strong>Conclusions: </strong>The combination of COP + RAP during self-expanding TAVI improves postoperative screening for conduction disturbances, thus reducing the need for cardiac rhythm monitoring, and the length stay. The COP + RAP strategy improves the short-term clinical outcomes of self-expanding TAVI due to fewer infection-related readmissions.</p>","PeriodicalId":34295,"journal":{"name":"REC Interventional Cardiology","volume":"7 2","pages":"82-90"},"PeriodicalIF":1.1000,"publicationDate":"2025-03-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12118476/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"REC Interventional Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.24875/RECIC.M24000497","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction and objectives: Because of the potential need for permanent pacemaker implantation, patients are frequently monitored for days after transcatheter aortic valve implantation (TAVI), particularly when using self-expanding valves. We sought to determine whether the appearance and management of conduction disturbances after TAVI can be improved by combining the cusp overlap projection (COP) and a rapid atrial pacing (RAP) protocol to detect the need for pacemaker implantation.
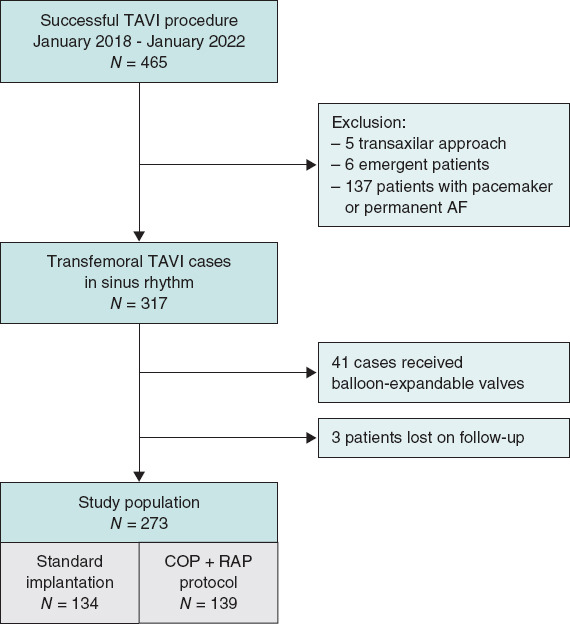
Methods: We consecutively studied a total of 273 patients who underwent TAVI with self-expanding valves from 2018 through 2022 (134 undergoing standard implantations and 139 COP + RAP). Assessment included the 90-day follow-up.
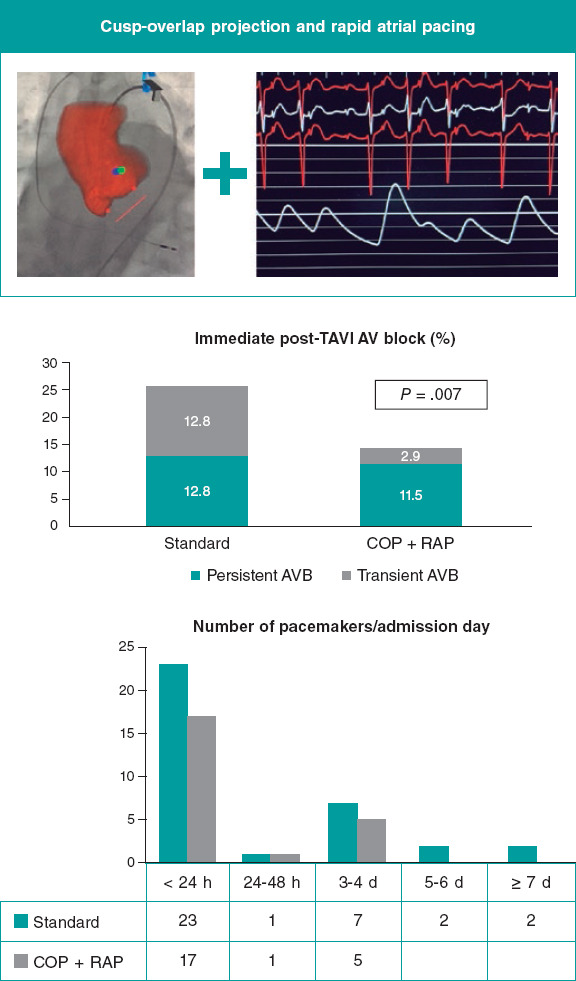
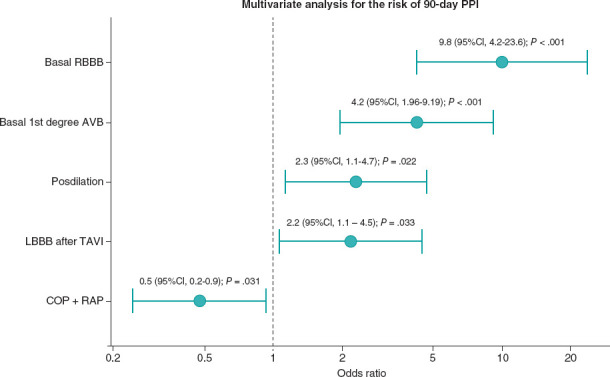
Results: Complete heart block was reported in 25.4% and 14.4% in the standard-of-care and COP + RAP group, with a marked decrease in transient atrioventricular block (12.8% vs 2.9%, respectively; P = .007). The absence of the Wenckebach phenomenon during RAP had a negative predictive value of 97% (95%CI, 91-99) for pacemaker implantation at the follow-up, which significantly decreased the need for 24-hour temporary pacemaker monitoring in the COP + RAP group (91.8% vs 28.1%; P < .0001) and the median [IQR] length of stay (5.0 [4-8] days vs 2.0 [1-4] days; P < .0001). At the 90-day follow-up, COP + RAP reduced pacemaker implantation (OR, 0.48; 95%CI, 0.24-0.92; P = .031), as well as the risk of infection-related readmissions significantly (OR, 0.35; 95%CI, 0.12-0.89; P = .036).
Conclusions: The combination of COP + RAP during self-expanding TAVI improves postoperative screening for conduction disturbances, thus reducing the need for cardiac rhythm monitoring, and the length stay. The COP + RAP strategy improves the short-term clinical outcomes of self-expanding TAVI due to fewer infection-related readmissions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


