{"title":"Fentanyl may not be necessary for adequate endoscopic moderate sedation.","authors":"Greg S Cohen, Kwang-Youn A Kim","doi":"10.4253/wjge.v17.i5.105031","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Although the majority of gastrointestinal (GI) endoscopies in the United States are now performed with propofol sedation, a substantial minority are performed with midazolam and fentanyl sedation. Despite the ubiquity of conscious sedation with midazolam and fentanyl in the United States, there is scant evidence specifically supporting the superiority of midazolam plus fentanyl over single agent midazolam sedation in GI endoscopy. We hypothesize that single agent sedation with midazolam is noninferior to sedation with midazolam plus fentanyl in GI endoscopy.</p><p><strong>Aim: </strong>To investigate whether sedation with midazolam alone is noninferior to sedation with midazolam plus fentanyl in GI endoscopy.</p><p><strong>Methods: </strong>We conducted a randomized, single-blind study to compare the safety and effectiveness of single agent midazolam vs. standard fentanyl/midazolam moderate sedation in 300 outpatients presenting for upper endoscopy and/or colonoscopy at a tertiary care hospital. Primary outcomes were patient satisfaction as measured by the previously validated Procedural Sedation Assessment Survey. Secondary outcomes were procedure quality measures and adverse events. Statistical analysis was performed by a biomedical statistician using the <i>χ</i> <sup>2</sup> test, Fisher's exact test, and Welch's 2-sample <i>t</i>-test.</p><p><strong>Results: </strong>There was no difference in patient satisfaction between sedation groups, as measured by a less than 1 point difference between groups in Procedural Sedation Assessment Survey scores for discomfort during the procedure, and for preference for level of sedation with future procedures. There were no differences in adverse events or procedure quality measures. Cecal intubation time was 1 minute longer in the single agent midazolam group, and an average of 2.7 mg more midazolam was administered when fentanyl was not included in the sedation regimen. The recruitment goal of 772 patients was not reached.</p><p><strong>Conclusion: </strong>It may be possible to minimize or avoid using fentanyl in endoscopist administered moderate sedation for GI endoscopy. We hope these findings spur further work in this under-researched area.</p>","PeriodicalId":23953,"journal":{"name":"World Journal of Gastrointestinal Endoscopy","volume":"17 5","pages":"105031"},"PeriodicalIF":1.8000,"publicationDate":"2025-05-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12110154/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4253/wjge.v17.i5.105031","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Although the majority of gastrointestinal (GI) endoscopies in the United States are now performed with propofol sedation, a substantial minority are performed with midazolam and fentanyl sedation. Despite the ubiquity of conscious sedation with midazolam and fentanyl in the United States, there is scant evidence specifically supporting the superiority of midazolam plus fentanyl over single agent midazolam sedation in GI endoscopy. We hypothesize that single agent sedation with midazolam is noninferior to sedation with midazolam plus fentanyl in GI endoscopy.
Aim: To investigate whether sedation with midazolam alone is noninferior to sedation with midazolam plus fentanyl in GI endoscopy.
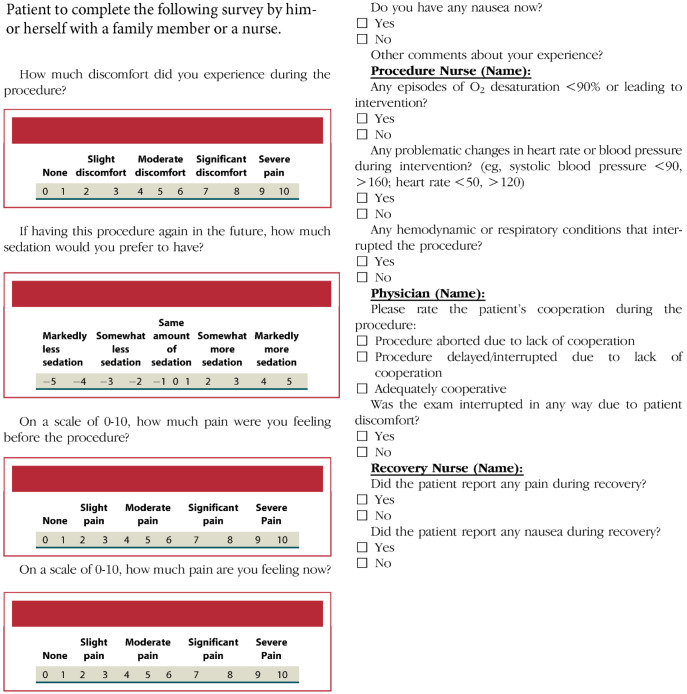
Methods: We conducted a randomized, single-blind study to compare the safety and effectiveness of single agent midazolam vs. standard fentanyl/midazolam moderate sedation in 300 outpatients presenting for upper endoscopy and/or colonoscopy at a tertiary care hospital. Primary outcomes were patient satisfaction as measured by the previously validated Procedural Sedation Assessment Survey. Secondary outcomes were procedure quality measures and adverse events. Statistical analysis was performed by a biomedical statistician using the χ2 test, Fisher's exact test, and Welch's 2-sample t-test.
Results: There was no difference in patient satisfaction between sedation groups, as measured by a less than 1 point difference between groups in Procedural Sedation Assessment Survey scores for discomfort during the procedure, and for preference for level of sedation with future procedures. There were no differences in adverse events or procedure quality measures. Cecal intubation time was 1 minute longer in the single agent midazolam group, and an average of 2.7 mg more midazolam was administered when fentanyl was not included in the sedation regimen. The recruitment goal of 772 patients was not reached.
Conclusion: It may be possible to minimize or avoid using fentanyl in endoscopist administered moderate sedation for GI endoscopy. We hope these findings spur further work in this under-researched area.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


