Late Graft Failure Due to Arterio-Venous Fistula in the Free Jejunal Graft Mesentery Following Total Pharyngo-Laryngo-Esophagectomy for Cervical Esophageal Cancer: A Case Report.
{"title":"Late Graft Failure Due to Arterio-Venous Fistula in the Free Jejunal Graft Mesentery Following Total Pharyngo-Laryngo-Esophagectomy for Cervical Esophageal Cancer: A Case Report.","authors":"Koutarou Yamamoto, Tomoyuki Okumura, Takeshi Miwa, Yoshihisa Numata, Tatsuhiro Araki, Ayaka Itoh, Mina Fukasawa, Nana Kimura, Masakazu Nagamori, Kosuke Mori, Naoya Takeda, Tomohiro Minagawa, Kenta Sukegawa, Toru Watanabe, Katsuhisa Hirano, Isaya Hashimoto, Kazuto Shibuya, Isaku Yoshioka, Hideharu Abe, Toshihiko Satake, Noriko Okuno, Tsutomu Fujii","doi":"10.70352/scrj.cr.25-0147","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Insufficient blood supply to free jejunal grafts after total pharyngo-laryngo-esophagectomy (TPLE) occurs primarily due to failure of the vascular anastomosis, often resulting in rapid graft necrosis. This report details a case of ischemic enteritis caused by an arteriovenous fistula (AVF) in the mesentery of the free jejunal graft, resulting in chronic stenosis and total removal of the jejunal graft.</p><p><strong>Case presentation: </strong>A 61-year-old woman diagnosed with squamous cell carcinoma of the cervical and thoracic esophagus underwent TPLE with gastric conduit and free jejunal graft reconstruction. The third jejunal artery and vein were anastomosed to the left transverse cervical artery and the internal jugular vein, respectively. On postoperative day (POD) 9, leakage was observed at the free jejunal-gastric anastomosis. The fistula healed with conservative treatment but a stenosis at the pharyngeal-jejunal anastomosis developed. Endoscopic observation after balloon dilation of the stenosis showed mucosal hemorrhage and ulcer scarring in the jejunal graft. A 3D reconstructed contrast-enhanced CT revealed the presence of an AVF in the free jejunal mesentery despite well-preserved blood flow across the vascular anastomosis. As no local inflammation was observed in the neck, and oral intake was sufficient after balloon dilatation, she was discharged from hospital. Seven months after surgery, she was admitted to our hospital due to obstruction of the pharyngeal-jejunal anastomosis with cutaneous fistula. Based on the disease course and endoscopic findings of the free jejunal graft, she was diagnosed with cutaneous fistula with scarring obstruction following chronic ischemic enteritis, considered difficult to heal with conservative treatment. Total removal of the free jejunum and reconstruction with an antero-lateral femoral thigh (ALT) flap was performed at 8 months after initial surgery. Oral intake was allowed on POD13, and she was discharged in good condition on POD30.</p><p><strong>Conclusions: </strong>We report here a rare case of late graft failure after TPLE due to chronic ischemia from an AVF in the mesentery of the free jejunal graft. Detailed assessment of mesenteric blood flow by 3D-constructed contrast-enhanced CT is useful and early removal of the ischemic jejunal graft is suggested.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"11 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12119138/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.70352/scrj.cr.25-0147","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/24 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Insufficient blood supply to free jejunal grafts after total pharyngo-laryngo-esophagectomy (TPLE) occurs primarily due to failure of the vascular anastomosis, often resulting in rapid graft necrosis. This report details a case of ischemic enteritis caused by an arteriovenous fistula (AVF) in the mesentery of the free jejunal graft, resulting in chronic stenosis and total removal of the jejunal graft.
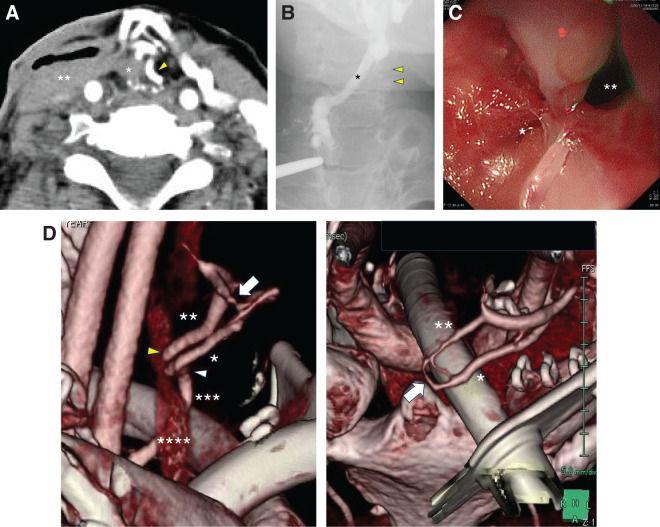
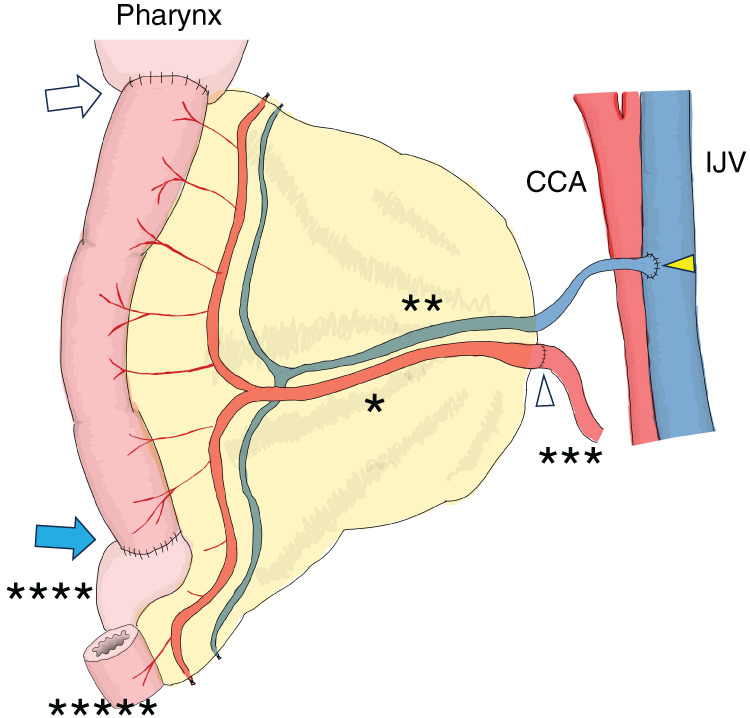
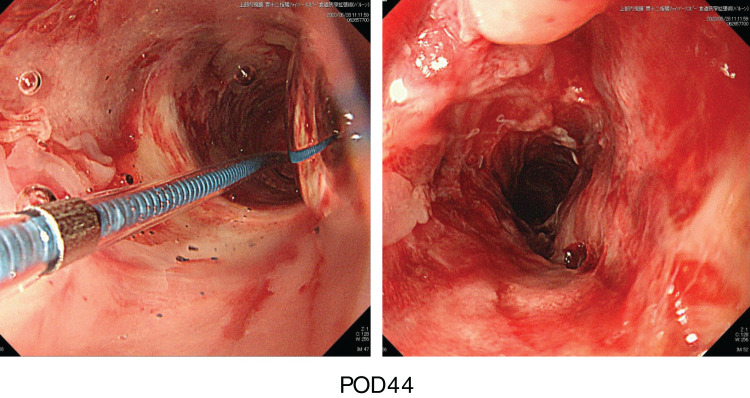
Case presentation: A 61-year-old woman diagnosed with squamous cell carcinoma of the cervical and thoracic esophagus underwent TPLE with gastric conduit and free jejunal graft reconstruction. The third jejunal artery and vein were anastomosed to the left transverse cervical artery and the internal jugular vein, respectively. On postoperative day (POD) 9, leakage was observed at the free jejunal-gastric anastomosis. The fistula healed with conservative treatment but a stenosis at the pharyngeal-jejunal anastomosis developed. Endoscopic observation after balloon dilation of the stenosis showed mucosal hemorrhage and ulcer scarring in the jejunal graft. A 3D reconstructed contrast-enhanced CT revealed the presence of an AVF in the free jejunal mesentery despite well-preserved blood flow across the vascular anastomosis. As no local inflammation was observed in the neck, and oral intake was sufficient after balloon dilatation, she was discharged from hospital. Seven months after surgery, she was admitted to our hospital due to obstruction of the pharyngeal-jejunal anastomosis with cutaneous fistula. Based on the disease course and endoscopic findings of the free jejunal graft, she was diagnosed with cutaneous fistula with scarring obstruction following chronic ischemic enteritis, considered difficult to heal with conservative treatment. Total removal of the free jejunum and reconstruction with an antero-lateral femoral thigh (ALT) flap was performed at 8 months after initial surgery. Oral intake was allowed on POD13, and she was discharged in good condition on POD30.
Conclusions: We report here a rare case of late graft failure after TPLE due to chronic ischemia from an AVF in the mesentery of the free jejunal graft. Detailed assessment of mesenteric blood flow by 3D-constructed contrast-enhanced CT is useful and early removal of the ischemic jejunal graft is suggested.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


