Giovanni Mantelli, Armando Fiore, Caterina Barberi, Barbara Zaia, Giorgio Ricci, Massimo Carollo, Fabio Malalan
{"title":"Severe Presentation of Cannabinoid Hyperemesis Syndrome With Mixed Acid-Base Disorder and Cardiac Complications: A Case Report.","authors":"Giovanni Mantelli, Armando Fiore, Caterina Barberi, Barbara Zaia, Giorgio Ricci, Massimo Carollo, Fabio Malalan","doi":"10.1155/carm/8161294","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Cannabinoid hyperemesis syndrome (CHS) is a condition characterized by cyclic abdominal pain, vomiting, and nausea, primarily affecting adolescents and adults with a history of chronic cannabis use. The diagnosis of CHS is clinical, with symptom resolution upon cannabis cessation considered pathognomonic. The overlap of CHS symptoms with other conditions complicates the differential diagnosis, particularly in emergency settings. <b>Case Presentation:</b> We report an unusual case of a 28-year-old man admitted to the Emergency Department of Rovereto (Italy) with limb paresthesia and agitation. Initial evaluation revealed indirect clinical signs of hypocalcemia, and QTc prolongation and severe hypokalemia on electrocardiogram. The arterial blood gas analysis suggested mixed acid-base disturbances. His symptoms improved with aggressive electrolyte correction, benzodiazepine administration, magnesium sulfate administration, and fluid resuscitation. Given the significant risk of arrhythmias, antiemetics known to prolong QTc, such as dopamine antagonists, were contraindicated, and midazolam was used as an alternative for symptom control (both nausea and agitation). <b>Conclusion:</b> This case underscores the importance of recognizing CHS as a potential etiology in patients with recurrent vomiting and a history of chronic cannabis use, even in the presence of atypical findings such as profound electrolyte imbalances and cardiac abnormalities. Given the protracted recovery period associated with CHS, early identification and patient education regarding cannabis cessation are crucial in preventing recurrent episodes.</p>","PeriodicalId":9627,"journal":{"name":"Case Reports in Medicine","volume":"2025 ","pages":"8161294"},"PeriodicalIF":0.7000,"publicationDate":"2025-05-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12119160/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/carm/8161294","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
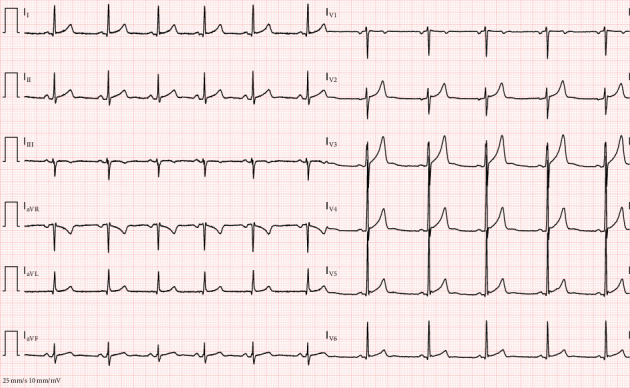
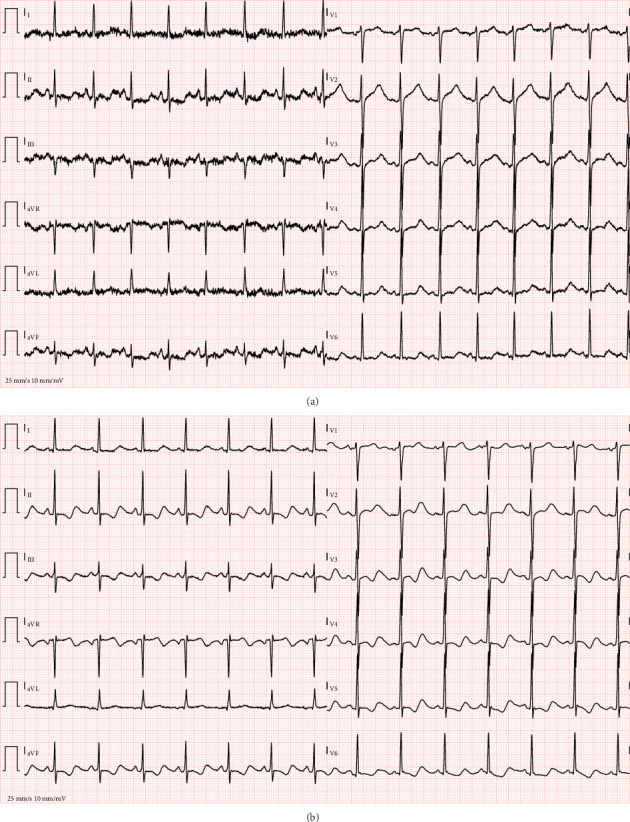
Background: Cannabinoid hyperemesis syndrome (CHS) is a condition characterized by cyclic abdominal pain, vomiting, and nausea, primarily affecting adolescents and adults with a history of chronic cannabis use. The diagnosis of CHS is clinical, with symptom resolution upon cannabis cessation considered pathognomonic. The overlap of CHS symptoms with other conditions complicates the differential diagnosis, particularly in emergency settings. Case Presentation: We report an unusual case of a 28-year-old man admitted to the Emergency Department of Rovereto (Italy) with limb paresthesia and agitation. Initial evaluation revealed indirect clinical signs of hypocalcemia, and QTc prolongation and severe hypokalemia on electrocardiogram. The arterial blood gas analysis suggested mixed acid-base disturbances. His symptoms improved with aggressive electrolyte correction, benzodiazepine administration, magnesium sulfate administration, and fluid resuscitation. Given the significant risk of arrhythmias, antiemetics known to prolong QTc, such as dopamine antagonists, were contraindicated, and midazolam was used as an alternative for symptom control (both nausea and agitation). Conclusion: This case underscores the importance of recognizing CHS as a potential etiology in patients with recurrent vomiting and a history of chronic cannabis use, even in the presence of atypical findings such as profound electrolyte imbalances and cardiac abnormalities. Given the protracted recovery period associated with CHS, early identification and patient education regarding cannabis cessation are crucial in preventing recurrent episodes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


