Javier Iglesias-Varea, Mario Fernández-Ruiz, Laura Domínguez, Jorge Boán, Eduardo Aparicio-Minguijón, Antonio Terrón, María Asunción Pérez-Jacoiste Asín, José María Aguado, Francisco López-Medrano
{"title":"[Impact of a dedicated multidisciplinary committee (<i>endocarditis team</i>) on the management and outcome of infective endocarditis in a reference center].","authors":"Javier Iglesias-Varea, Mario Fernández-Ruiz, Laura Domínguez, Jorge Boán, Eduardo Aparicio-Minguijón, Antonio Terrón, María Asunción Pérez-Jacoiste Asín, José María Aguado, Francisco López-Medrano","doi":"10.37201/req/020.2025","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Infective endocarditis (IE) is a complex condition associated with high morbidity and mortality. The creation of multidisciplinary teams (endocarditis team) has been shown to improve its management and prognosis. We analysed the impact of the formal implementation of a multidisciplinary IE committee (coIE) in a tertiary care hospital.</p><p><strong>Methods: </strong>Single-centre quasi-experimental study comparing two periods: before (2010-2015) and after (2017-2021) the implementation of the coIE. The coIE met weekly (and on demand when necessary) to make decisions regarding medical and surgical management in patients with definite or possible IE, following a protocol based on international guidelines.</p><p><strong>Results: </strong>We included 92 and 97 patients in the pre- and post-intervention periods, respectively. Demographic characteristics, predisposing factors, and types of IE were similar. No significant differences were observed in the proportion of patients with surgical indication who underwent surgery (30.2 % vs 39.1 %, respectively; p = 0.317), in-hospital mortality (27.2 % vs 34.0 %; p = 0.308), or one-year mortality (32.6 % vs 45.4 %; p = 0.073). The median (interquartile range) time from diagnosis to surgery decreased in the post-intervention period (11.5 [6.3-25.3] vs 7 [3-10] days; p = 0.026). The diagnosis of embolic events was more frequent in this period (46.7 % vs 58.8 %; p = 0.098).</p><p><strong>Conclusions: </strong>Although we did not observe a significant impact on mortality among patients with definite IE after the implementation of an endocarditis team, we noted a favourable trend in intermediate indicators of healthcare quality.</p>","PeriodicalId":94198,"journal":{"name":"Revista espanola de quimioterapia : publicacion oficial de la Sociedad Espanola de Quimioterapia","volume":" ","pages":"294-304"},"PeriodicalIF":2.2000,"publicationDate":"2025-05-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12257183/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Revista espanola de quimioterapia : publicacion oficial de la Sociedad Espanola de Quimioterapia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.37201/req/020.2025","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Infective endocarditis (IE) is a complex condition associated with high morbidity and mortality. The creation of multidisciplinary teams (endocarditis team) has been shown to improve its management and prognosis. We analysed the impact of the formal implementation of a multidisciplinary IE committee (coIE) in a tertiary care hospital.
Methods: Single-centre quasi-experimental study comparing two periods: before (2010-2015) and after (2017-2021) the implementation of the coIE. The coIE met weekly (and on demand when necessary) to make decisions regarding medical and surgical management in patients with definite or possible IE, following a protocol based on international guidelines.
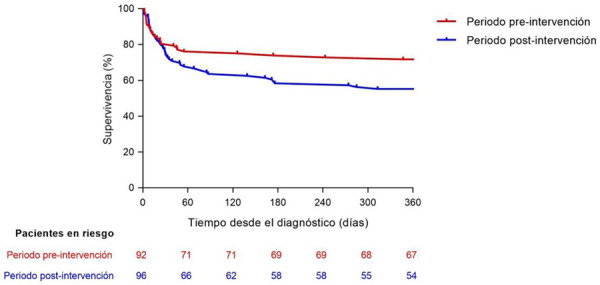
Results: We included 92 and 97 patients in the pre- and post-intervention periods, respectively. Demographic characteristics, predisposing factors, and types of IE were similar. No significant differences were observed in the proportion of patients with surgical indication who underwent surgery (30.2 % vs 39.1 %, respectively; p = 0.317), in-hospital mortality (27.2 % vs 34.0 %; p = 0.308), or one-year mortality (32.6 % vs 45.4 %; p = 0.073). The median (interquartile range) time from diagnosis to surgery decreased in the post-intervention period (11.5 [6.3-25.3] vs 7 [3-10] days; p = 0.026). The diagnosis of embolic events was more frequent in this period (46.7 % vs 58.8 %; p = 0.098).
Conclusions: Although we did not observe a significant impact on mortality among patients with definite IE after the implementation of an endocarditis team, we noted a favourable trend in intermediate indicators of healthcare quality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


