Emily N Jenkins, Jeremy A W Gold, Kaitlin Benedict, Shawn R Lockhart, Elizabeth L Berkow, Tamia Dixon, Shanita L Shack, Lucy S Witt, Lee H Harrison, Shannon Seopaul, Maria A Correa, Megan Fitzsimons, Yalda Jabarkhyl, Devra Barter, Christopher A Czaja, Helen Johnston, Tiffanie Markus, William Schaffner, Annastasia Gross, Ruth Lynfield, Laura Tourdot, Joelle Nadle, Jeremy Roland, Gabriela Escutia, Alexia Y Zhang, Anita Gellert, Christine Hurley, Brenda L Tesini, Erin C Phipps, Sarah Shrum Davis, Meghan Lyman
{"title":"Population-Based Active Surveillance for Culture-Confirmed Candidemia - 10 Sites, United States, 2017-2021.","authors":"Emily N Jenkins, Jeremy A W Gold, Kaitlin Benedict, Shawn R Lockhart, Elizabeth L Berkow, Tamia Dixon, Shanita L Shack, Lucy S Witt, Lee H Harrison, Shannon Seopaul, Maria A Correa, Megan Fitzsimons, Yalda Jabarkhyl, Devra Barter, Christopher A Czaja, Helen Johnston, Tiffanie Markus, William Schaffner, Annastasia Gross, Ruth Lynfield, Laura Tourdot, Joelle Nadle, Jeremy Roland, Gabriela Escutia, Alexia Y Zhang, Anita Gellert, Christine Hurley, Brenda L Tesini, Erin C Phipps, Sarah Shrum Davis, Meghan Lyman","doi":"10.15585/mmwr.ss7404a1","DOIUrl":null,"url":null,"abstract":"<p><strong>Problem/condition: </strong>Candidemia, a bloodstream infection caused by Candida spp., is a common cause of health care-associated bloodstream infections in the United States. Candidemia is associated with substantial health care costs, morbidity, and mortality.</p><p><strong>Period covered: </strong>2017-2021.</p><p><strong>Description of system: </strong>CDC's Emerging Infections Program (EIP), a collaboration among CDC, state health departments, and academic partners, was used to conduct active, population-based laboratory surveillance for candidemia at city or county sites located in 10 states (California, Colorado, Connecticut, Georgia, Maryland, Minnesota, New Mexico, New York, Oregon, and Tennessee), representing a combined population of approximately 21.5 million persons, or 7% of the U.S. population in 2019. Connecticut began reporting cases on January 1, 2019, and conducts statewide surveillance. Although candidemia is not a nationally notifiable condition, cases of Candida auris infection are nationally notifiable, and cases of candidemia caused by C. auris could be included in both national case counts and EIP surveillance. A culture-confirmed candidemia case is defined as a positive blood culture for any Candida sp. from a resident in the surveillance catchment area. Subsequent positive blood cultures for Candida within 30 days of the initial positive culture (index date) in the same patient are considered part of the same case. Clinical laboratories serving each catchment area report candidemia cases, and trained surveillance officers abstract information from medical charts for all cases. Corresponding isolates are sent to CDC for species confirmation and antifungal susceptibility testing.</p><p><strong>Results: </strong>A total of 7,381 candidemia cases were identified during the surveillance period (2017-2021). The overall incidence was 7.4 cases per 100,000 population. Across age groups, sexes, racial and ethnic groups, and surveillance sites, incidence was generally stable or increased slightly from 2017 to 2021, with the lowest overall incidence in 2019 (6.8) and the highest in 2021 (7.9). In 2021, candidemia incidence was highest in patients aged ≥65 years (22.7) and infants (aged <1 year) (8.0). Incidence was higher in males (8.7) compared with females (7.0) and higher in non-Hispanic Black or African American (Black) patients (12.8) compared with non-Black patients (5.6). Incidence was highest in Maryland (14.5), followed by Tennessee (10.1) and Georgia (10.0); incidence was lowest in Oregon (4.8). Increases occurred in the percentage of cases classified as health care onset (52.2% in 2017 to 58.0% in 2021). Overall, among 7,381 cases (in 6,235 patients), 63.7% occurred in patients who had a central venous catheter, 80.7% involved recent systemic antibiotic receipt, and 9.0% occurred in patients who had a history of injection drug use. The percentage of cases with a positive SARS-CoV-2 test during the 90 days before or after the index date increased from 10.4% in 2020 to 17.7% in 2021. From 2017 to 2021, the percentage of cases involving an intensive care unit stay before the index date increased from 38.3% to 44.9%. Echinocandins (e.g., micafungin) were used as treatment in 49.8% of cases, and azoles were used in 47.7%. The all-cause in-hospital mortality rate was 32.6%; this increased from 26.8% in 2019 to 36.1% in 2021. Overall, Candida albicans accounted for 37.1% of cases, followed by Candida glabrata (30.4%) and Candida parapsilosis (13.5%); however, C. glabrata was the most frequent species in California (38.4%) and Maryland (32.9%). Candida auris infections accounted for 0.4% of cases. Among 6,576 Candida isolates for which interpretive breakpoints exist and isolates were available for testing, 5.6% were fluconazole resistant, and <1% were echinocandin resistant. Antifungal resistance was stable for all antifungals tested across years.</p><p><strong>Interpretation: </strong>Candidemia remains an important health care-associated infection. The disproportionate incidence among older adults, males, and Black patients is consistent with previous reports, and the overall incidence of candidemia has not changed substantially compared with previous EIP findings based on data collected during 2012-2016 (8.7 per 100,000 population). The higher mortality rate associated with candidemia during 2020-2021 likely reflects consequences of the COVID-19 pandemic, including strained health care systems and an increased population of patients who were susceptible to candidemia because of COVID-19-related critical illness.</p><p><strong>Public health action: </strong>Strict implementation of measures to prevent health care-associated bloodstream infections is important to help prevent candidemia cases. Health care officials and providers should be vigilant for candidemia as a complication of critical illness. Continued surveillance is needed to monitor for emerging populations at risk for candidemia and changes in antifungal resistance patterns, which can help guide antifungal treatment selection.</p>","PeriodicalId":48549,"journal":{"name":"Mmwr Surveillance Summaries","volume":"74 4","pages":"1-15"},"PeriodicalIF":49.8000,"publicationDate":"2025-05-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12115505/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mmwr Surveillance Summaries","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.15585/mmwr.ss7404a1","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Problem/condition: Candidemia, a bloodstream infection caused by Candida spp., is a common cause of health care-associated bloodstream infections in the United States. Candidemia is associated with substantial health care costs, morbidity, and mortality.
Period covered: 2017-2021.
Description of system: CDC's Emerging Infections Program (EIP), a collaboration among CDC, state health departments, and academic partners, was used to conduct active, population-based laboratory surveillance for candidemia at city or county sites located in 10 states (California, Colorado, Connecticut, Georgia, Maryland, Minnesota, New Mexico, New York, Oregon, and Tennessee), representing a combined population of approximately 21.5 million persons, or 7% of the U.S. population in 2019. Connecticut began reporting cases on January 1, 2019, and conducts statewide surveillance. Although candidemia is not a nationally notifiable condition, cases of Candida auris infection are nationally notifiable, and cases of candidemia caused by C. auris could be included in both national case counts and EIP surveillance. A culture-confirmed candidemia case is defined as a positive blood culture for any Candida sp. from a resident in the surveillance catchment area. Subsequent positive blood cultures for Candida within 30 days of the initial positive culture (index date) in the same patient are considered part of the same case. Clinical laboratories serving each catchment area report candidemia cases, and trained surveillance officers abstract information from medical charts for all cases. Corresponding isolates are sent to CDC for species confirmation and antifungal susceptibility testing.
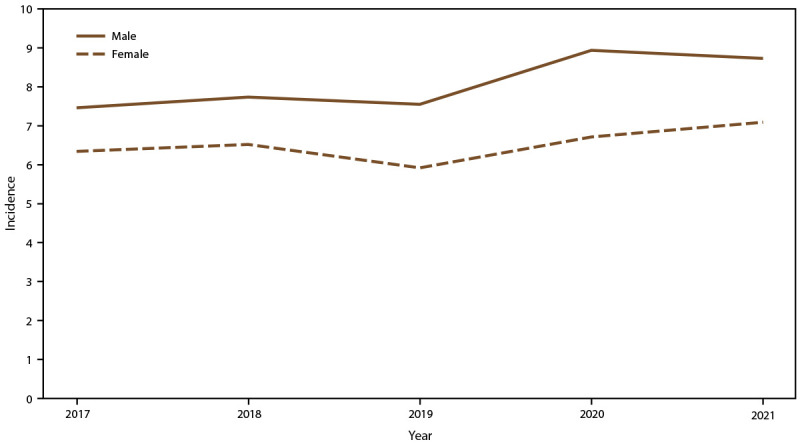
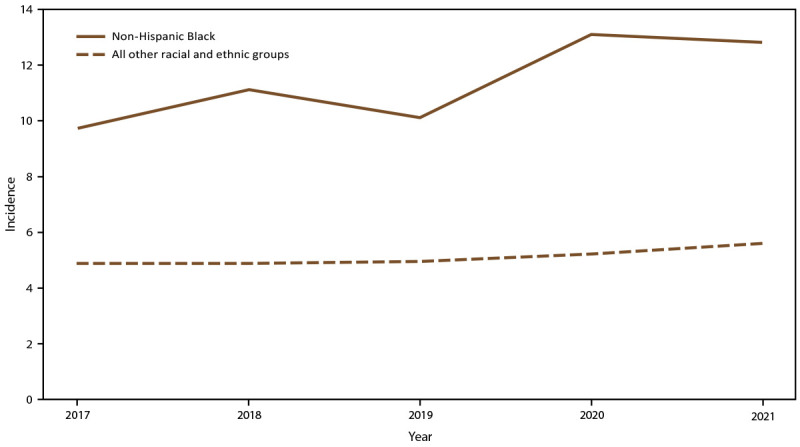
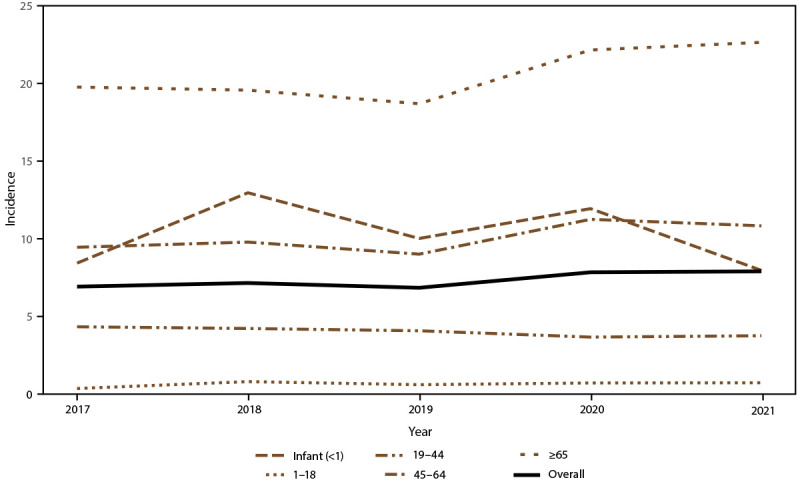
Results: A total of 7,381 candidemia cases were identified during the surveillance period (2017-2021). The overall incidence was 7.4 cases per 100,000 population. Across age groups, sexes, racial and ethnic groups, and surveillance sites, incidence was generally stable or increased slightly from 2017 to 2021, with the lowest overall incidence in 2019 (6.8) and the highest in 2021 (7.9). In 2021, candidemia incidence was highest in patients aged ≥65 years (22.7) and infants (aged <1 year) (8.0). Incidence was higher in males (8.7) compared with females (7.0) and higher in non-Hispanic Black or African American (Black) patients (12.8) compared with non-Black patients (5.6). Incidence was highest in Maryland (14.5), followed by Tennessee (10.1) and Georgia (10.0); incidence was lowest in Oregon (4.8). Increases occurred in the percentage of cases classified as health care onset (52.2% in 2017 to 58.0% in 2021). Overall, among 7,381 cases (in 6,235 patients), 63.7% occurred in patients who had a central venous catheter, 80.7% involved recent systemic antibiotic receipt, and 9.0% occurred in patients who had a history of injection drug use. The percentage of cases with a positive SARS-CoV-2 test during the 90 days before or after the index date increased from 10.4% in 2020 to 17.7% in 2021. From 2017 to 2021, the percentage of cases involving an intensive care unit stay before the index date increased from 38.3% to 44.9%. Echinocandins (e.g., micafungin) were used as treatment in 49.8% of cases, and azoles were used in 47.7%. The all-cause in-hospital mortality rate was 32.6%; this increased from 26.8% in 2019 to 36.1% in 2021. Overall, Candida albicans accounted for 37.1% of cases, followed by Candida glabrata (30.4%) and Candida parapsilosis (13.5%); however, C. glabrata was the most frequent species in California (38.4%) and Maryland (32.9%). Candida auris infections accounted for 0.4% of cases. Among 6,576 Candida isolates for which interpretive breakpoints exist and isolates were available for testing, 5.6% were fluconazole resistant, and <1% were echinocandin resistant. Antifungal resistance was stable for all antifungals tested across years.
Interpretation: Candidemia remains an important health care-associated infection. The disproportionate incidence among older adults, males, and Black patients is consistent with previous reports, and the overall incidence of candidemia has not changed substantially compared with previous EIP findings based on data collected during 2012-2016 (8.7 per 100,000 population). The higher mortality rate associated with candidemia during 2020-2021 likely reflects consequences of the COVID-19 pandemic, including strained health care systems and an increased population of patients who were susceptible to candidemia because of COVID-19-related critical illness.
Public health action: Strict implementation of measures to prevent health care-associated bloodstream infections is important to help prevent candidemia cases. Health care officials and providers should be vigilant for candidemia as a complication of critical illness. Continued surveillance is needed to monitor for emerging populations at risk for candidemia and changes in antifungal resistance patterns, which can help guide antifungal treatment selection.
期刊介绍:
The Morbidity and Mortality Weekly Report (MMWR) Series, produced by the Centers for Disease Control and Prevention (CDC), is commonly referred to as "the voice of CDC." Serving as the primary outlet for timely, reliable, authoritative, accurate, objective, and practical public health information and recommendations, the MMWR is a crucial publication. Its readership primarily includes physicians, nurses, public health practitioners, epidemiologists, scientists, researchers, educators, and laboratorians.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


