Qin Wang, Ruoya Wang, Jianze Wang, Na Sai, Shuhang Fan, Jianbin Sun, Zhikai Zhao, Junhui Huang, Weidong Shen, Weiju Han
{"title":"Outcome of different facial nerve managements in petrous bone cholesteatoma patients with facial paralysis.","authors":"Qin Wang, Ruoya Wang, Jianze Wang, Na Sai, Shuhang Fan, Jianbin Sun, Zhikai Zhao, Junhui Huang, Weidong Shen, Weiju Han","doi":"10.1186/s13005-025-00520-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Active Facial nerve (FN) management, including decompression, end-to-end or rerouting anastomosis, and grafting consistently plays an important role in the surgical management of petrous bone cholesteatoma (PBC), and postoperative FN function is also a major concern for surgeons. The aim of this study is to analyze the long-term FN function outcomes in PBC patients with FN paralysis who have underwent different managements and to explore the prognostic factors.</p><p><strong>Methods: </strong>A retrospective analysis of 160 PBC patients with preoperative FN paralysis was conducted, and long-term FN function outcome was evaluated. Multivariate ordinal logistic regression models were used to determine the prognostic factors.</p><p><strong>Results: </strong>160 patients were collected. 102 males (63.75%) and 58 females (36.25%) with mean age 34.09 ± 13.54 years (range: 5.58-77 years). Mean FN paralysis duration preoperatively was 62.5 ± 90.80 months (range: 4 days-46 years). The preoperative/postoperative House-Brackmann (H-B) grade are as follows: H-B (I-II): 0/38 cases, H-B III: 11/37 cases, H-B IV: 22/38 cases, H-B V: 21/14 cases.</p><p><strong>H-b vi: </strong>106/33 cases. The poorer preoperative FN function, the poorer postoperative FN function (r<sub>s</sub>=0.745, P < 0.001). Among 160 PBC patients, 127 patients underwent active FN management, 94/127 (74.0%) with preoperative H-B (V-VI) improved postoperatively. 33 patients were not eligible for FN repair, due to prolonged period of complete FN paralysis. FN decompression achieved H-B (I-II) recovery in 100% of H-B (III-IV) patients (22/22) within 12 months of paralysis and 88.9% (8/9) of H-B (V-VI) patients operated within 2 months of paralysis. End-to-end/rerouting anastomosis achieved H-B III recovery in 77.8% (14/18) of patients treated within 12 months. Greater auricular nerve graft within 12 months of paralysis achieved H-B III recovery in 75% of patients. Hypoglossal-FN anastomosis yielded H-B IV recovery in 7/12 patients (58.3%). Multivariate analysis identified worse preoperative FN function and prolonged FN paralysis duration (P < 0.05) as independent risk factors for poor prognosis.</p><p><strong>Conclusions: </strong>Patients with FN paralysis can undergo active FN management to reconstruct FN function, depending on the preoperative FN function and the duration of FN paralysis. Worse preoperative FN function and longer duration of FN paralysis (P < 0.05) are risk factors for poorer prognosis.</p>","PeriodicalId":12994,"journal":{"name":"Head & Face Medicine","volume":"21 1","pages":"42"},"PeriodicalIF":2.4000,"publicationDate":"2025-05-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12117717/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Head & Face Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13005-025-00520-x","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"DENTISTRY, ORAL SURGERY & MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Active Facial nerve (FN) management, including decompression, end-to-end or rerouting anastomosis, and grafting consistently plays an important role in the surgical management of petrous bone cholesteatoma (PBC), and postoperative FN function is also a major concern for surgeons. The aim of this study is to analyze the long-term FN function outcomes in PBC patients with FN paralysis who have underwent different managements and to explore the prognostic factors.
Methods: A retrospective analysis of 160 PBC patients with preoperative FN paralysis was conducted, and long-term FN function outcome was evaluated. Multivariate ordinal logistic regression models were used to determine the prognostic factors.
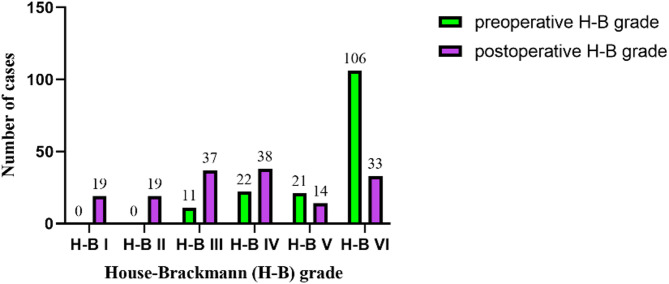
Results: 160 patients were collected. 102 males (63.75%) and 58 females (36.25%) with mean age 34.09 ± 13.54 years (range: 5.58-77 years). Mean FN paralysis duration preoperatively was 62.5 ± 90.80 months (range: 4 days-46 years). The preoperative/postoperative House-Brackmann (H-B) grade are as follows: H-B (I-II): 0/38 cases, H-B III: 11/37 cases, H-B IV: 22/38 cases, H-B V: 21/14 cases.
H-b vi: 106/33 cases. The poorer preoperative FN function, the poorer postoperative FN function (rs=0.745, P < 0.001). Among 160 PBC patients, 127 patients underwent active FN management, 94/127 (74.0%) with preoperative H-B (V-VI) improved postoperatively. 33 patients were not eligible for FN repair, due to prolonged period of complete FN paralysis. FN decompression achieved H-B (I-II) recovery in 100% of H-B (III-IV) patients (22/22) within 12 months of paralysis and 88.9% (8/9) of H-B (V-VI) patients operated within 2 months of paralysis. End-to-end/rerouting anastomosis achieved H-B III recovery in 77.8% (14/18) of patients treated within 12 months. Greater auricular nerve graft within 12 months of paralysis achieved H-B III recovery in 75% of patients. Hypoglossal-FN anastomosis yielded H-B IV recovery in 7/12 patients (58.3%). Multivariate analysis identified worse preoperative FN function and prolonged FN paralysis duration (P < 0.05) as independent risk factors for poor prognosis.
Conclusions: Patients with FN paralysis can undergo active FN management to reconstruct FN function, depending on the preoperative FN function and the duration of FN paralysis. Worse preoperative FN function and longer duration of FN paralysis (P < 0.05) are risk factors for poorer prognosis.
期刊介绍:
Head & Face Medicine is a multidisciplinary open access journal that publishes basic and clinical research concerning all aspects of cranial, facial and oral conditions.
The journal covers all aspects of cranial, facial and oral diseases and their management. It has been designed as a multidisciplinary journal for clinicians and researchers involved in the diagnostic and therapeutic aspects of diseases which affect the human head and face. The journal is wide-ranging, covering the development, aetiology, epidemiology and therapy of head and face diseases to the basic science that underlies these diseases. Management of head and face diseases includes all aspects of surgical and non-surgical treatments including psychopharmacological therapies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


