Mahmoud Balata, Tetsu Tanaka, Atsushi Sugiura, Refik Kavsur, Johanna Vogelhuber, Can Öztürk, Sebastian Zimmer, Julian Luetkens, Georg Nickenig, Marcel Weber
{"title":"Association between psoas muscle area and outcomes after transcatheter tricuspid valve repair.","authors":"Mahmoud Balata, Tetsu Tanaka, Atsushi Sugiura, Refik Kavsur, Johanna Vogelhuber, Can Öztürk, Sebastian Zimmer, Julian Luetkens, Georg Nickenig, Marcel Weber","doi":"10.1007/s12928-025-01136-3","DOIUrl":null,"url":null,"abstract":"<p><p>Transcatheter tricuspid valve repair (TTVR) might be an alternative option to reduce tricuspid regurgitation (TR) in patients with sarcopenia. Psoas muscle area (PMA) measured using computed tomography (CT) is known as a marker of sarcopenia. We investigated the association of PMA with procedural and clinical outcomes following TTVR. We retrospectively measured left and right PMA using pre-procedural CT in patients undergoing TTVR. Low PMA was defined as the total PMA < 20.3 cm<sup>2</sup> for men and < 11.8 cm<sup>2</sup> for women. The primary outcome was a composite of all-cause mortality and heart failure hospitalization within one year after TTVR. Of 163 patients, 47 (29%) were considered as having low PMA. Procedural success, defined as residual TR of ≤ 2 + at discharge, and in-hospital mortality were comparable between patients with low and high PMA. Patients with low PMA had a higher incidence of the composite outcome than those with high PMA (49% vs. 21%; p = 0.001) This association was consistent after adjusting for baseline characteristics (adjusted hazard ratio 0.43; 95% confidence interval: 0.23-0.80; p = 0.008). In contrast, the New York Heart Association functional class improved from baseline to three-month follow-up, regardless of PMA. Approximately 30% of patients undergoing TTVR were found to have low PMA. Although TTVR may be a safe therapeutic option to reduce TR and improve heart failure symptoms in patients with sarcopenia, the prognosis after TTVR remains poor in this population. Pre-procedural CT-based assessment of PMA may enhance risk stratification and support better clinical decision-making for TTVR.</p>","PeriodicalId":9439,"journal":{"name":"Cardiovascular Intervention and Therapeutics","volume":" ","pages":"679-688"},"PeriodicalIF":5.8000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12167307/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular Intervention and Therapeutics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s12928-025-01136-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/27 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
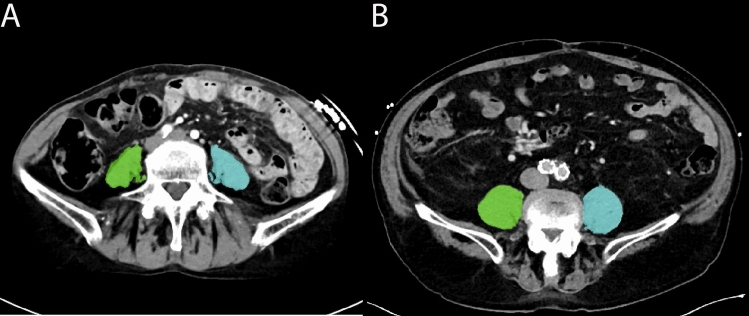
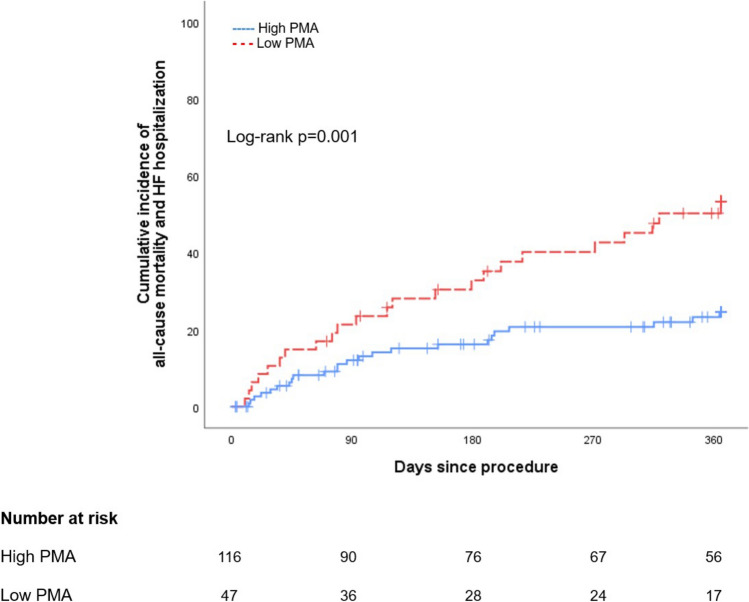
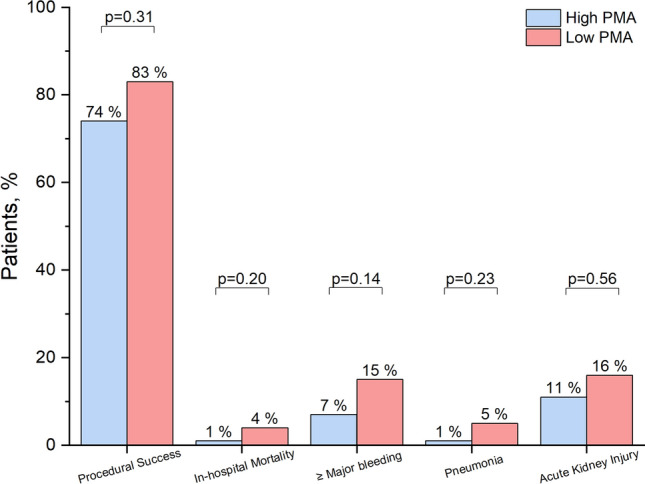
Transcatheter tricuspid valve repair (TTVR) might be an alternative option to reduce tricuspid regurgitation (TR) in patients with sarcopenia. Psoas muscle area (PMA) measured using computed tomography (CT) is known as a marker of sarcopenia. We investigated the association of PMA with procedural and clinical outcomes following TTVR. We retrospectively measured left and right PMA using pre-procedural CT in patients undergoing TTVR. Low PMA was defined as the total PMA < 20.3 cm2 for men and < 11.8 cm2 for women. The primary outcome was a composite of all-cause mortality and heart failure hospitalization within one year after TTVR. Of 163 patients, 47 (29%) were considered as having low PMA. Procedural success, defined as residual TR of ≤ 2 + at discharge, and in-hospital mortality were comparable between patients with low and high PMA. Patients with low PMA had a higher incidence of the composite outcome than those with high PMA (49% vs. 21%; p = 0.001) This association was consistent after adjusting for baseline characteristics (adjusted hazard ratio 0.43; 95% confidence interval: 0.23-0.80; p = 0.008). In contrast, the New York Heart Association functional class improved from baseline to three-month follow-up, regardless of PMA. Approximately 30% of patients undergoing TTVR were found to have low PMA. Although TTVR may be a safe therapeutic option to reduce TR and improve heart failure symptoms in patients with sarcopenia, the prognosis after TTVR remains poor in this population. Pre-procedural CT-based assessment of PMA may enhance risk stratification and support better clinical decision-making for TTVR.
期刊介绍:
Cardiovascular Intervention and Therapeutics (CVIT) is an international journal covering the field of cardiovascular disease and includes cardiac (coronary and noncoronary) and peripheral interventions and therapeutics. Articles are subject to peer review and complete editorial evaluation prior to any decision regarding acceptability. CVIT is an official journal of The Japanese Association of Cardiovascular Intervention and Therapeutics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


