Emily Wang, Abdelhamid Aboghanem, Niki Dacouris, Lindita Rapi, Sami Mahmud, Weiqiu Yuan, Rosane Nisenbaum, Michelle M Nash, G V Ramesh Prasad
{"title":"C-Reactive Protein Monitoring Identifies Urinary Tract Infections in Ambulatory Kidney Transplant Recipients.","authors":"Emily Wang, Abdelhamid Aboghanem, Niki Dacouris, Lindita Rapi, Sami Mahmud, Weiqiu Yuan, Rosane Nisenbaum, Michelle M Nash, G V Ramesh Prasad","doi":"10.1177/20543581251342428","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Urinary tract infections (UTI) are common in kidney transplant recipients (KTR). Although risk factors for UTI are well described, predicting symptomatic UTI with positive urine cultures in the first posttransplant year is challenging.</p><p><strong>Objective: </strong>Our clinic routinely monitors serum highly sensitive C-reactive protein (CRP) as part of posttransplant care. We sought to define the role of CRP in identifying symptomatic UTI in KTR.</p><p><strong>Design: </strong>Nested case control study.</p><p><strong>Setting: </strong>A large adult single-organ kidney transplant center in Toronto, Canada.</p><p><strong>Patients: </strong>We identified a nested cohort of 78 KTR who experienced a symptomatic UTI with positive urine cultures (cases) and compared them to a cohort of 78 KTR controls matched by time elapsed posttransplant.</p><p><strong>Measurements: </strong>Patient demographics, urine cultures, CRP, and kidney function during the first posttransplant year.</p><p><strong>Methods: </strong>We identified a cohort of KTR transplanted between January 1, 2016, and December 31, 2019. A positive urine culture ordered only for clinical indication in the first posttransplant year identified KTR with a UTI defined >10 <sup>5</sup> colony forming units/mL. UTI cases were matched 1:1 to non-UTI controls transplanted immediately preceding or succeeding the UTI case. Bivariate comparisons were performed by <i>t</i> test, Wilcoxon 2-sample test for continuous variables, chi-square, or Fisher's exact test as appropriate, with clinically significant variables entered into multivariable logistic regression models to determine associations.</p><p><strong>Results: </strong>Older age, female sex, and the presence of a stent were each associated with a UTI. Immediately preceding UTI, eGFR (<i>P</i> = .019), serum albumin (<i>P</i> < .0001), and hemoglobin (<i>P</i> = .002) were lower, while serum CRP (<i>P</i> < .0001) and absolute neutrophils (<i>P</i> = .03) were higher in cases than controls. However, in several multivariable models, only absolute CRP (<i>P</i> = .001), change in CRP (<i>P</i> = .005), female sex (<i>P</i> < .0001), and ureteric stent (<i>P</i> = .008) consistently predicted a UTI. Each 5 mg/dL change between the 2 preceding CRP values predicted a 15% increased likelihood of UTI, while each 1 mg/dL in absolute CRP concentration was associated with a 5% risk.</p><p><strong>Limitations: </strong>Retrospective case-control design, single-center, small sample size. Hospital inpatients and patients with other infections, acute inflammatory conditions, or rejection were excluded. Urine infections may more easily be detected when patients visit the clinic frequently.</p><p><strong>Conclusions: </strong>Routine ambulatory CRP monitoring in the first year may help identify subsequent symptomatic UTI in KTR, allow for the initiation of earlier therapy, and reduce patient morbidity.</p><p><strong>What was known before?: </strong>UTI in KTR are common in the first posttransplant year. Antibiotic therapy is typically not initiated until the results of urine cultures become known.</p><p><strong>What this adds: </strong>The routine use of appropriate biomarkers such as CRP as part of a posttransplant monitoring strategy may allow clinicians to order urine cultures, help identify UTI earlier, and start therapy sooner, promoting patient well-being.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"12 ","pages":"20543581251342428"},"PeriodicalIF":1.5000,"publicationDate":"2025-05-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12103657/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581251342428","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Urinary tract infections (UTI) are common in kidney transplant recipients (KTR). Although risk factors for UTI are well described, predicting symptomatic UTI with positive urine cultures in the first posttransplant year is challenging.
Objective: Our clinic routinely monitors serum highly sensitive C-reactive protein (CRP) as part of posttransplant care. We sought to define the role of CRP in identifying symptomatic UTI in KTR.
Design: Nested case control study.
Setting: A large adult single-organ kidney transplant center in Toronto, Canada.
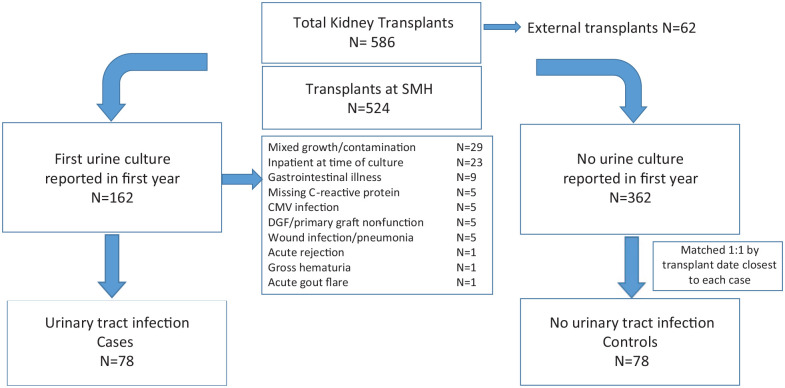
Patients: We identified a nested cohort of 78 KTR who experienced a symptomatic UTI with positive urine cultures (cases) and compared them to a cohort of 78 KTR controls matched by time elapsed posttransplant.
Measurements: Patient demographics, urine cultures, CRP, and kidney function during the first posttransplant year.
Methods: We identified a cohort of KTR transplanted between January 1, 2016, and December 31, 2019. A positive urine culture ordered only for clinical indication in the first posttransplant year identified KTR with a UTI defined >10 5 colony forming units/mL. UTI cases were matched 1:1 to non-UTI controls transplanted immediately preceding or succeeding the UTI case. Bivariate comparisons were performed by t test, Wilcoxon 2-sample test for continuous variables, chi-square, or Fisher's exact test as appropriate, with clinically significant variables entered into multivariable logistic regression models to determine associations.
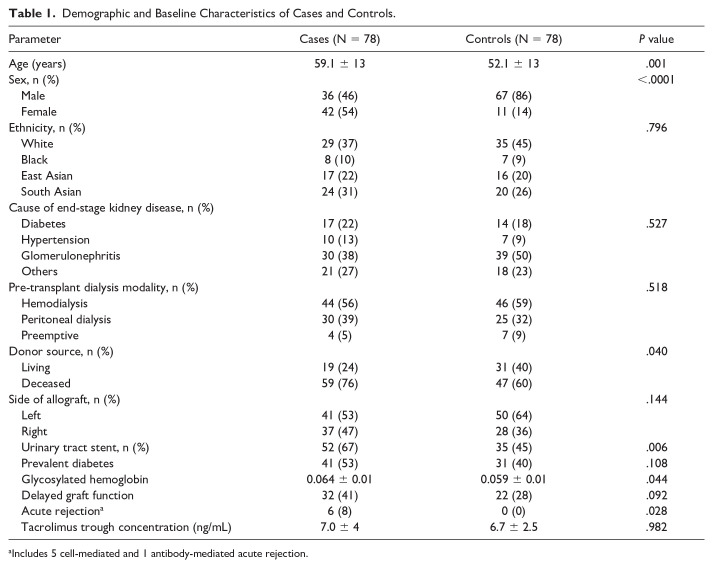
Results: Older age, female sex, and the presence of a stent were each associated with a UTI. Immediately preceding UTI, eGFR (P = .019), serum albumin (P < .0001), and hemoglobin (P = .002) were lower, while serum CRP (P < .0001) and absolute neutrophils (P = .03) were higher in cases than controls. However, in several multivariable models, only absolute CRP (P = .001), change in CRP (P = .005), female sex (P < .0001), and ureteric stent (P = .008) consistently predicted a UTI. Each 5 mg/dL change between the 2 preceding CRP values predicted a 15% increased likelihood of UTI, while each 1 mg/dL in absolute CRP concentration was associated with a 5% risk.
Limitations: Retrospective case-control design, single-center, small sample size. Hospital inpatients and patients with other infections, acute inflammatory conditions, or rejection were excluded. Urine infections may more easily be detected when patients visit the clinic frequently.
Conclusions: Routine ambulatory CRP monitoring in the first year may help identify subsequent symptomatic UTI in KTR, allow for the initiation of earlier therapy, and reduce patient morbidity.
What was known before?: UTI in KTR are common in the first posttransplant year. Antibiotic therapy is typically not initiated until the results of urine cultures become known.
What this adds: The routine use of appropriate biomarkers such as CRP as part of a posttransplant monitoring strategy may allow clinicians to order urine cultures, help identify UTI earlier, and start therapy sooner, promoting patient well-being.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


