Maria Califano, Jacopo Pruccoli, Oliviero Cavallino, Alessandra Lenzi, Antonia Parmeggiani
{"title":"Psychopathological Comorbidities in Children and Adolescents with Feeding and Eating Disorders: An Italian Clinical Study.","authors":"Maria Califano, Jacopo Pruccoli, Oliviero Cavallino, Alessandra Lenzi, Antonia Parmeggiani","doi":"10.3390/pediatric17030061","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Feeding and eating disorders (FED) represent a major public health issue and are the second leading cause of death among psychiatric conditions in children and adolescents. Psychopathological comorbidities play a significant role in the onset and persistence of FED, yet research on their underlying structure remains limited. This study explores the psychiatric comorbidities associated with FED, focusing on common etiopathogenetic factors and their clinical implications.</p><p><strong>Methods: </strong>Data were retrospectively collected from the Italian Regional Center for FED in the Emilia-Romagna Region between June 2023 and April 2024. Diagnoses were assigned following DSM-5 criteria using the Italian version of the semi-structured K-SADS-PL diagnostic interview. Principal component analysis (PCA) was performed to identify latent psychological dimensions underlying FED psychopathology, retaining five components based on the scree plot. Additionally, an analysis of covariance (ANCOVA) was conducted to examine differences in factor scores across FED subtypes, while adjusting for potential confounders.</p><p><strong>Results: </strong>Seventy-two participants were included (mean age: 14.6 years; mean BMI: 18.3 kg/m<sup>2</sup>; male-to-female ratio: 1:8). Diagnoses were distributed as follows: 63.9% anorexia nervosa (AN), 13.9% other specified feeding and eating disorder (OSFED), 6.9% avoidant restrictive food intake disorder (ARFID), 4.2% binge eating disorder (BED), 4.2% unspecified feeding and eating disorder (UFED), and 2.7% bulimia nervosa (BN). All participants met the criteria for at least one psychiatric comorbidity. Identified psychopathological clusters include the following: (1) mood disorders (66.5%); (2) anxiety disorders (87.5%); (3) obsessive-compulsive and related disorders (47.2%); (4) neurodevelopmental disorders, i.e., attention-deficit/hyperactivity disorder (ADHD) (30.5%); (5) disruptive and impulse-control disorders (13.9%); and (6) psychotic symptoms (40.3%). No instances of tic or elimination disorders were detected. Conduct disorder was more prevalent among UFED, BED, and BN patients compared to other FED (<i>p</i> = 0.005), and moderate/severe ADHD was associated with higher body mass index (BMI) (<i>p</i> = 0.035). PCA revealed distinct psychological dimensions underlying FED, while ANCOVA indicated significant differences in factor scores across FED subtypes, supporting the presence of shared transdiagnostic mechanisms.</p><p><strong>Conclusions: </strong>This study highlights the complex interplay between FED and psychiatric comorbidities, emphasizing the need for early intervention and personalized treatment approaches. The dimensional structure identified through PCA suggests that common psychopathological factors may drive FED development, and ANCOVA findings support their differential expression across FED types. Future research should further investigate these transdiagnostic mechanisms to optimize clinical care.</p>","PeriodicalId":45251,"journal":{"name":"Pediatric Reports","volume":"17 3","pages":""},"PeriodicalIF":1.4000,"publicationDate":"2025-05-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12101277/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/pediatric17030061","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Feeding and eating disorders (FED) represent a major public health issue and are the second leading cause of death among psychiatric conditions in children and adolescents. Psychopathological comorbidities play a significant role in the onset and persistence of FED, yet research on their underlying structure remains limited. This study explores the psychiatric comorbidities associated with FED, focusing on common etiopathogenetic factors and their clinical implications.
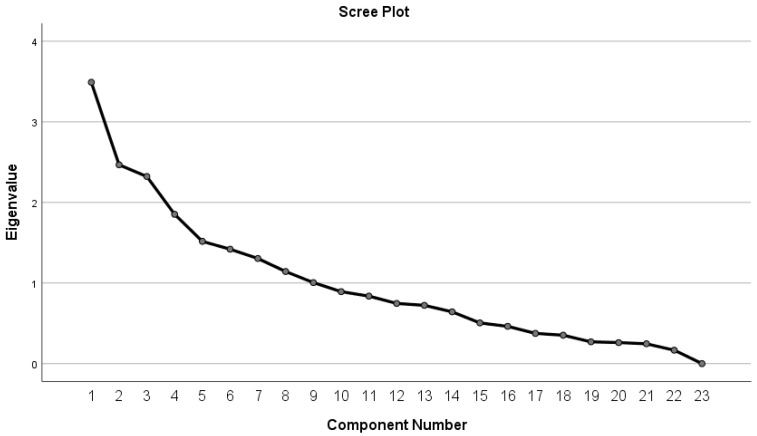
Methods: Data were retrospectively collected from the Italian Regional Center for FED in the Emilia-Romagna Region between June 2023 and April 2024. Diagnoses were assigned following DSM-5 criteria using the Italian version of the semi-structured K-SADS-PL diagnostic interview. Principal component analysis (PCA) was performed to identify latent psychological dimensions underlying FED psychopathology, retaining five components based on the scree plot. Additionally, an analysis of covariance (ANCOVA) was conducted to examine differences in factor scores across FED subtypes, while adjusting for potential confounders.
Results: Seventy-two participants were included (mean age: 14.6 years; mean BMI: 18.3 kg/m2; male-to-female ratio: 1:8). Diagnoses were distributed as follows: 63.9% anorexia nervosa (AN), 13.9% other specified feeding and eating disorder (OSFED), 6.9% avoidant restrictive food intake disorder (ARFID), 4.2% binge eating disorder (BED), 4.2% unspecified feeding and eating disorder (UFED), and 2.7% bulimia nervosa (BN). All participants met the criteria for at least one psychiatric comorbidity. Identified psychopathological clusters include the following: (1) mood disorders (66.5%); (2) anxiety disorders (87.5%); (3) obsessive-compulsive and related disorders (47.2%); (4) neurodevelopmental disorders, i.e., attention-deficit/hyperactivity disorder (ADHD) (30.5%); (5) disruptive and impulse-control disorders (13.9%); and (6) psychotic symptoms (40.3%). No instances of tic or elimination disorders were detected. Conduct disorder was more prevalent among UFED, BED, and BN patients compared to other FED (p = 0.005), and moderate/severe ADHD was associated with higher body mass index (BMI) (p = 0.035). PCA revealed distinct psychological dimensions underlying FED, while ANCOVA indicated significant differences in factor scores across FED subtypes, supporting the presence of shared transdiagnostic mechanisms.
Conclusions: This study highlights the complex interplay between FED and psychiatric comorbidities, emphasizing the need for early intervention and personalized treatment approaches. The dimensional structure identified through PCA suggests that common psychopathological factors may drive FED development, and ANCOVA findings support their differential expression across FED types. Future research should further investigate these transdiagnostic mechanisms to optimize clinical care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


