Diego Alejandro Cubides-Diaz, Valentina Negrette-Lazaro, Viviana Poveda-Hurtado, Juan Pablo López-Salazar, Carlos Mauricio Calderón-Vargas, Carlos Arturo Álvarez-Moreno
{"title":"Bone Marrow Infection by <i>Pneumocystis jirovecii</i> in a Patient with AIDS: A Case Report and Literature Review.","authors":"Diego Alejandro Cubides-Diaz, Valentina Negrette-Lazaro, Viviana Poveda-Hurtado, Juan Pablo López-Salazar, Carlos Mauricio Calderón-Vargas, Carlos Arturo Álvarez-Moreno","doi":"10.3390/idr17030047","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong><i>Pneumocystis jirovecii</i> primarily causes pneumonia in immunosuppressed individuals, particularly those living with advanced HIV/AIDS. Extrapulmonary dissemination is uncommon, with bone marrow involvement described in only a handful of cases globally. Bone marrow infection occurs in the setting of severe immunosuppression, poses diagnostic challenges, and carries a high mortality rate.</p><p><strong>Methods: </strong>We describe the case of a 34-year-old man newly diagnosed with HIV/AIDS, presenting with severe immunosuppression and <i>Pneumocystis jirovecii</i> pneumonia. The patient initially improved with cotrimoxazole and corticosteroids, but was readmitted shortly after discharge with abdominal pain, diarrhea, and worsening pancytopenia. A bone marrow biopsy revealed <i>Pneumocystis jirovecii</i> cysts, confirming disseminated infection. Concomitant Kaposi sarcoma involving the skin and gastrointestinal tract was also diagnosed. Despite antimicrobial therapy, the patient's condition worsened, leading to multisystem organ failure and death two months later.</p><p><strong>Conclusions: </strong>This case highlights a rare presentation of disseminated <i>Pneumocystis jirovecii</i> infection with bone marrow involvement in a patient with advanced HIV/AIDS. Although infrequent, this complication should be considered in individuals with <i>Pneumocystis jirovecii</i> pneumonia who develop persistent cytopenias and systemic symptoms. Diagnosis depends on histopathologic confirmation, which may lead to under-recognition. Early suspicion and individualized management are essential, though the optimal treatment approach for extrapulmonary infection remains undefined.</p>","PeriodicalId":13579,"journal":{"name":"Infectious Disease Reports","volume":"17 3","pages":""},"PeriodicalIF":2.4000,"publicationDate":"2025-05-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12101389/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Disease Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/idr17030047","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Pneumocystis jirovecii primarily causes pneumonia in immunosuppressed individuals, particularly those living with advanced HIV/AIDS. Extrapulmonary dissemination is uncommon, with bone marrow involvement described in only a handful of cases globally. Bone marrow infection occurs in the setting of severe immunosuppression, poses diagnostic challenges, and carries a high mortality rate.
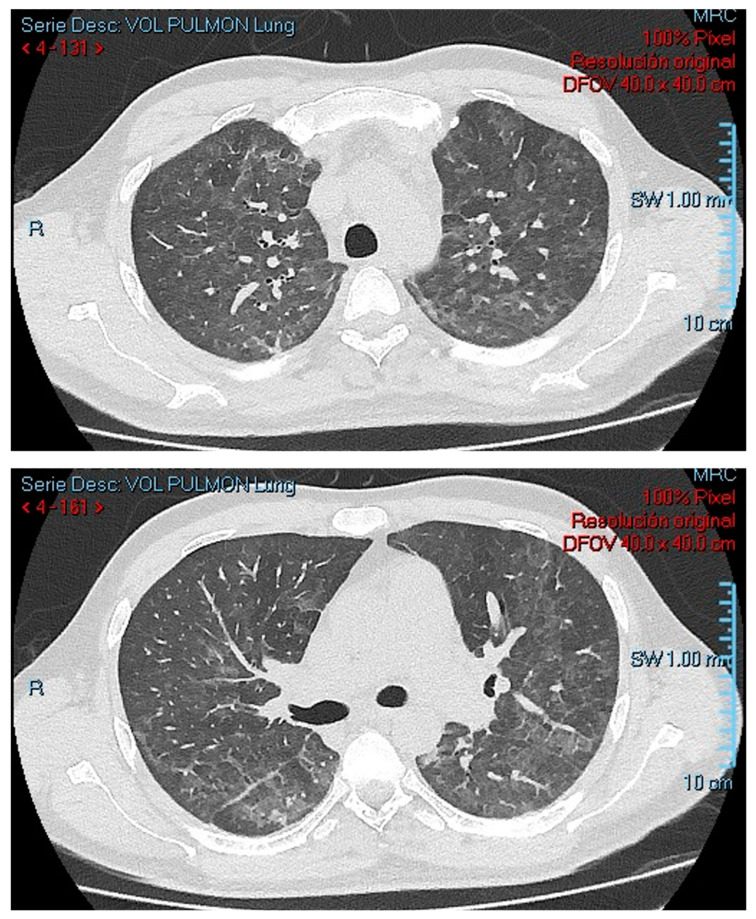
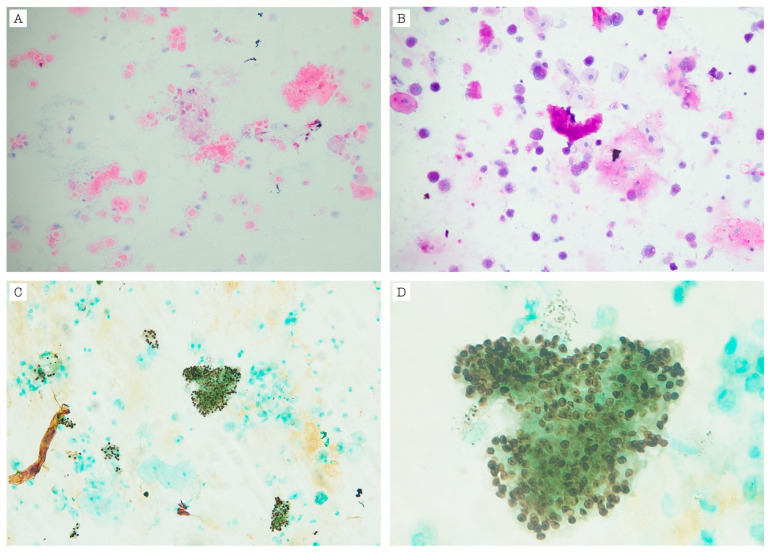
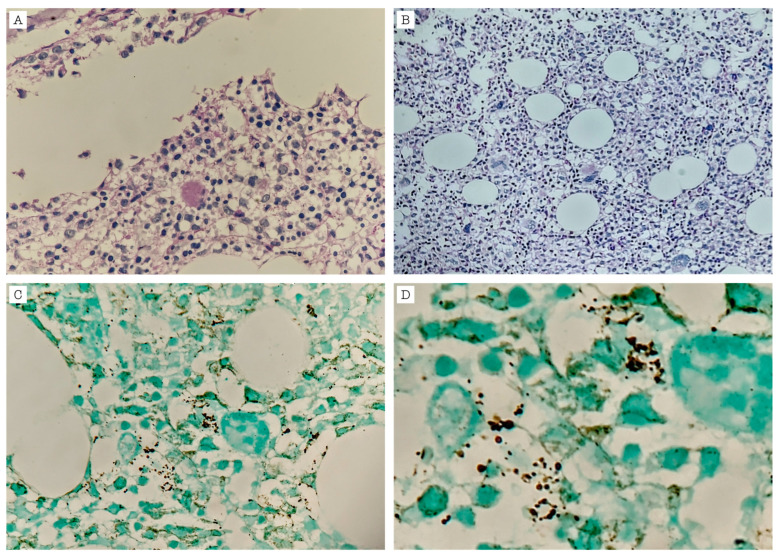
Methods: We describe the case of a 34-year-old man newly diagnosed with HIV/AIDS, presenting with severe immunosuppression and Pneumocystis jirovecii pneumonia. The patient initially improved with cotrimoxazole and corticosteroids, but was readmitted shortly after discharge with abdominal pain, diarrhea, and worsening pancytopenia. A bone marrow biopsy revealed Pneumocystis jirovecii cysts, confirming disseminated infection. Concomitant Kaposi sarcoma involving the skin and gastrointestinal tract was also diagnosed. Despite antimicrobial therapy, the patient's condition worsened, leading to multisystem organ failure and death two months later.
Conclusions: This case highlights a rare presentation of disseminated Pneumocystis jirovecii infection with bone marrow involvement in a patient with advanced HIV/AIDS. Although infrequent, this complication should be considered in individuals with Pneumocystis jirovecii pneumonia who develop persistent cytopenias and systemic symptoms. Diagnosis depends on histopathologic confirmation, which may lead to under-recognition. Early suspicion and individualized management are essential, though the optimal treatment approach for extrapulmonary infection remains undefined.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


