The Appearance of Osteomyelitis of the Foot and Disseminated Subcutaneous Abscesses During Treatment for Disseminated Tuberculosis Infection in an Immunocompetent Patient: Case Presentation of a Paradoxical Reaction and Literature Review.
Luca Santilli, Benedetta Canovari, Maria Balducci, Francesco Ginevri, Monia Maracci, Antonio Polenta, Norma Anzalone, Lucia Franca, Beatrice Mariotti, Lucia Sterza, Francesco Barchiesi
{"title":"The Appearance of Osteomyelitis of the Foot and Disseminated Subcutaneous Abscesses During Treatment for Disseminated Tuberculosis Infection in an Immunocompetent Patient: Case Presentation of a Paradoxical Reaction and Literature Review.","authors":"Luca Santilli, Benedetta Canovari, Maria Balducci, Francesco Ginevri, Monia Maracci, Antonio Polenta, Norma Anzalone, Lucia Franca, Beatrice Mariotti, Lucia Sterza, Francesco Barchiesi","doi":"10.3390/idr17030046","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> The appearance of new clinical manifestations (for example, subcutaneous or skin abscesses) during anti-tuberculosis treatment is generally indicative of therapeutic failure. The cause of therapeutic failure may be the presence of a drug-resistant <i>Mycobacterium</i> infection or to the failure to achieve a sufficient concentration of the drugs in the bloodstream. <b>Case report:</b> Here, we report the case of a 25-year-old man suffering from tuberculosis infection with lymph-node and pulmonary involvement and an atypical response to specific therapy. Two weeks after starting four-drug antitubercular treatment, the patient began to experience fever, pain and functional impotence in the left foot and ankle, with subsequent evidence of ankle and tarsal osteomyelitis. Four weeks after starting treatment, the patient presented with several widespread, painful subcutaneous abscesses on the trunk, back and right lower limb. Drainage was performed from the ankle and from one of the abscesses, and polymerase chain reaction (PCR) showed a positive result for <i>M. tuberculosis</i> in both samples, with the absence of resistance to drugs. Anti-tubercular medications were continued, with resolution of the pulmonary and bone involvement but with persistence of subcutaneous abscesses, although subsequent drainages showed the absence of mycobacterium tuberculosis. <b>Conclusions:</b> We describe an unusual presentation of paradoxical reaction in the form of osteomyelitis and subcutaneous abscesses in an immunocompetent TB patient, and we reported other similar cases of paradoxical reactions described in the literature in the last ten years, which demonstrate the importance of considering paradoxical reactions in patients who present with new or worsening signs and symptoms after starting tuberculosis treatment.</p>","PeriodicalId":13579,"journal":{"name":"Infectious Disease Reports","volume":"17 3","pages":""},"PeriodicalIF":2.4000,"publicationDate":"2025-05-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12101366/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Disease Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/idr17030046","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
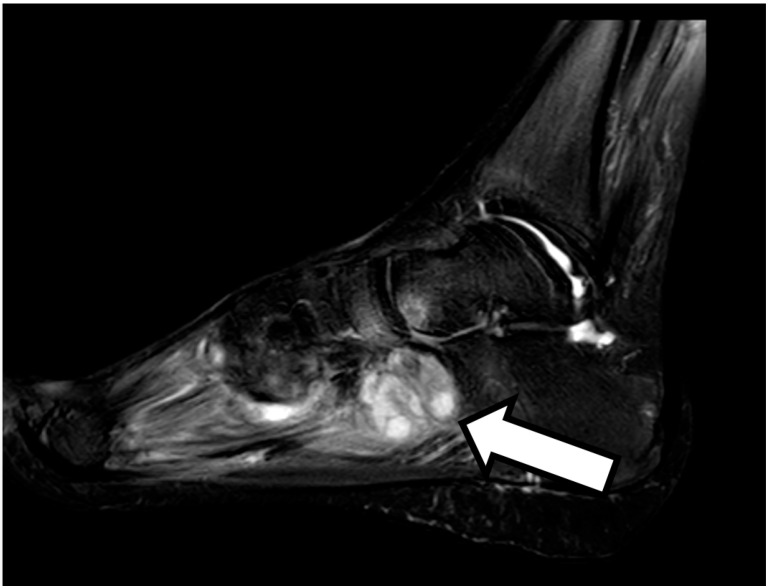
Background: The appearance of new clinical manifestations (for example, subcutaneous or skin abscesses) during anti-tuberculosis treatment is generally indicative of therapeutic failure. The cause of therapeutic failure may be the presence of a drug-resistant Mycobacterium infection or to the failure to achieve a sufficient concentration of the drugs in the bloodstream. Case report: Here, we report the case of a 25-year-old man suffering from tuberculosis infection with lymph-node and pulmonary involvement and an atypical response to specific therapy. Two weeks after starting four-drug antitubercular treatment, the patient began to experience fever, pain and functional impotence in the left foot and ankle, with subsequent evidence of ankle and tarsal osteomyelitis. Four weeks after starting treatment, the patient presented with several widespread, painful subcutaneous abscesses on the trunk, back and right lower limb. Drainage was performed from the ankle and from one of the abscesses, and polymerase chain reaction (PCR) showed a positive result for M. tuberculosis in both samples, with the absence of resistance to drugs. Anti-tubercular medications were continued, with resolution of the pulmonary and bone involvement but with persistence of subcutaneous abscesses, although subsequent drainages showed the absence of mycobacterium tuberculosis. Conclusions: We describe an unusual presentation of paradoxical reaction in the form of osteomyelitis and subcutaneous abscesses in an immunocompetent TB patient, and we reported other similar cases of paradoxical reactions described in the literature in the last ten years, which demonstrate the importance of considering paradoxical reactions in patients who present with new or worsening signs and symptoms after starting tuberculosis treatment.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


