Tagayasu Anzai, Kenji Hirata, Ken Kato, Kohsuke Kudo
{"title":"Machine learning for cardio-oncology: predicting global longitudinal strain from conventional echocardiographic measurements in cancer patients.","authors":"Tagayasu Anzai, Kenji Hirata, Ken Kato, Kohsuke Kudo","doi":"10.1186/s40959-025-00348-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Global longitudinal strain (GLS) is an important prognostic indicator for predicting heart failure and cancer therapy-related cardiac dysfunction (CTRCD). Although access to GLS measurement has increased across institutions, its actual use in clinical practice remains limited due to practical barriers such as limited time and insufficient training. If reduced GLS could be predicted from conventional echocardiographic parameters, it could help identify patients who would most benefit from direct GLS assessment. Therefore, in this study, we tested the hypothesis that reduced GLS can be predicted from conventional echocardiography via a machine learning (ML) approach.</p><p><strong>Methods: </strong>This single-center cross-sectional study included patients who visited the Tokyo Metropolitan Tama Medical Center Hospital and underwent echocardiography with GLS before or after anticancer chemotherapy. Low-GLS was defined as a GLS < 16; otherwise, it was defined as Normal-GLS. Patients with EF < 50% were excluded. We developed ML models that predict Low-GLS from conventional echocardiography measurements. Sixteen ML models were constructed including various boosting and tree-based methods. We assessed the models by the area under the receiver operating characteristic curve (AUC), accuracy, sensitivity, specificity, Positive predictive value (PPV), Negative predictive value (NPV), and F1 score. The Shapley Additive exPlanations (SHAP) method was employed to evaluate the essential predictors.</p><p><strong>Results: </strong>A total of 1,484 patients (64 ± 13 years old, 69% female) were enrolled for ML model development, including 406 patients with Low-GLS and 1,078 with Normal-GLS. The best model for the test dataset was the CatBoost classifier (AUC, 0.748; accuracy, 0.734). Diastolic dysfunction indices [such as septal/lateral mitral annular early diastolic velocity (e') and E-wave to atrial contraction filling velocity (E/A)] and peak velocity‑related parameters [aortic valve peak velocity (AV-Vmax) and left ventricular outflow tract velocity maximum (LVOT-Vmax)] played essential roles in the Low-GLS prediction model.</p><p><strong>Conclusion: </strong>This study indicated the possibility that Low-GLS might be predicted by machine learning models from conventional echocardiography measurements in cancer patients.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"11 1","pages":"49"},"PeriodicalIF":3.2000,"publicationDate":"2025-05-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12096611/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-025-00348-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Global longitudinal strain (GLS) is an important prognostic indicator for predicting heart failure and cancer therapy-related cardiac dysfunction (CTRCD). Although access to GLS measurement has increased across institutions, its actual use in clinical practice remains limited due to practical barriers such as limited time and insufficient training. If reduced GLS could be predicted from conventional echocardiographic parameters, it could help identify patients who would most benefit from direct GLS assessment. Therefore, in this study, we tested the hypothesis that reduced GLS can be predicted from conventional echocardiography via a machine learning (ML) approach.
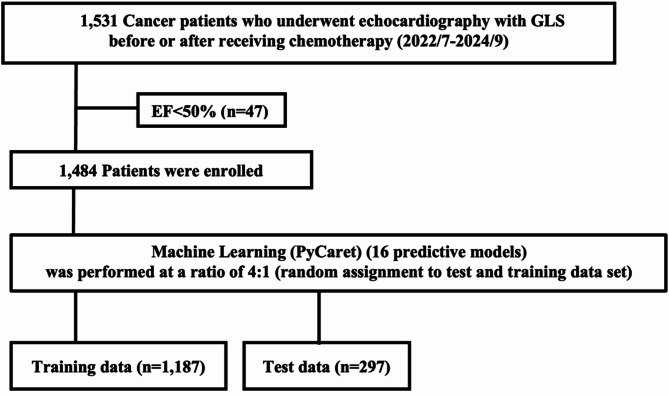
Methods: This single-center cross-sectional study included patients who visited the Tokyo Metropolitan Tama Medical Center Hospital and underwent echocardiography with GLS before or after anticancer chemotherapy. Low-GLS was defined as a GLS < 16; otherwise, it was defined as Normal-GLS. Patients with EF < 50% were excluded. We developed ML models that predict Low-GLS from conventional echocardiography measurements. Sixteen ML models were constructed including various boosting and tree-based methods. We assessed the models by the area under the receiver operating characteristic curve (AUC), accuracy, sensitivity, specificity, Positive predictive value (PPV), Negative predictive value (NPV), and F1 score. The Shapley Additive exPlanations (SHAP) method was employed to evaluate the essential predictors.
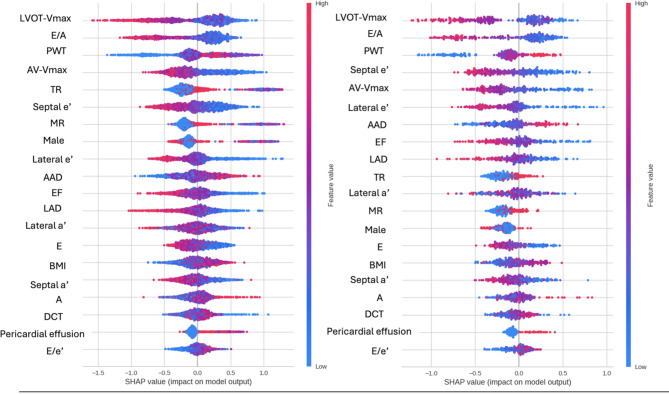
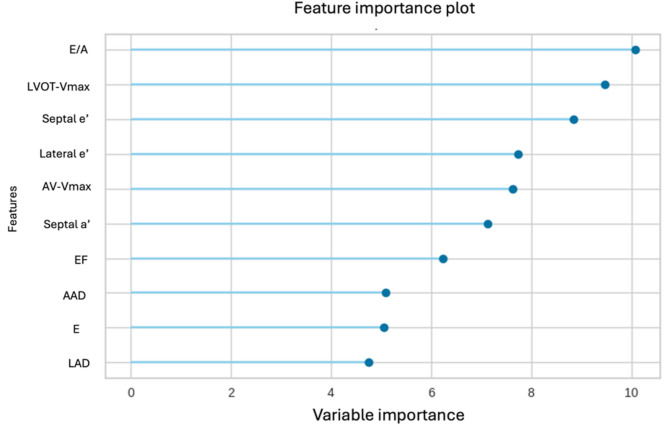
Results: A total of 1,484 patients (64 ± 13 years old, 69% female) were enrolled for ML model development, including 406 patients with Low-GLS and 1,078 with Normal-GLS. The best model for the test dataset was the CatBoost classifier (AUC, 0.748; accuracy, 0.734). Diastolic dysfunction indices [such as septal/lateral mitral annular early diastolic velocity (e') and E-wave to atrial contraction filling velocity (E/A)] and peak velocity‑related parameters [aortic valve peak velocity (AV-Vmax) and left ventricular outflow tract velocity maximum (LVOT-Vmax)] played essential roles in the Low-GLS prediction model.
Conclusion: This study indicated the possibility that Low-GLS might be predicted by machine learning models from conventional echocardiography measurements in cancer patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


