Gaurav Suryawanshi, Megan B Ghai, Nauroze Faizi, Stuart K Amateau, Nabeel Azeem, Shawn Mallery, Martin L Freeman, Guru Trikudanathan
{"title":"Predictors of 30-Day Unplanned Readmission in Necrotizing Pancreatitis: A 12-Year Experience From a Tertiary Care Center.","authors":"Gaurav Suryawanshi, Megan B Ghai, Nauroze Faizi, Stuart K Amateau, Nabeel Azeem, Shawn Mallery, Martin L Freeman, Guru Trikudanathan","doi":"10.14309/ctg.0000000000000848","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Hospital readmission rate is a key hospital metric and represents a substantial burden to patients and the healthcare system. Necrotizing pancreatitis (NP) patients are at high risk of unplanned readmission. The aim of this study was to determine the incidence and predictors of 30-day unplanned readmission after index hospitalization for NP.</p><p><strong>Methods: </strong>Adult NP patients who were managed at a single tertiary referral center between 2009 and 2022 were identified from a prospective database and categorized into 2 groups based on 30-day unplanned readmission after index hospitalization. Patients with no follow-up who died during index admission or within 30 days of discharge were excluded. Baseline data on admission including demographic, clinical, interventional, imaging, and discharge characteristics were compared. Multivariable analysis was completed to identify independent predictors of 30-day readmission.</p><p><strong>Results: </strong>Among 505 patients with NP (male patients-347 [69%], median age-50 years [inter quartile range 37-63]) 191 (37.8%) had at least 1 unplanned readmission. The most common causes of readmission were abdominal pain (40%) and sepsis (27%). On multivariable analysis, independent predictors for early readmission were necrosis collection size ≥ 6 cm (adjusted odds ratio [aOR] 1.91 [1.11-3.30], P < 0.03), stay at outside hospital ≥ 14 days before transfer to tertiary center (aOR 2.89 [1.27-6.60], P < 0.01), and need for percutaneous feeding tube at the time of discharge (aOR 2.06 [1.01-4.21], P < 0.05).</p><p><strong>Discussion: </strong>Readmission after NP is common and associated with greater mortality at 6 months. Expedited transfer to tertiary center for timely intervention, assiduous follow-up of other high-risk patients (large collections and those who need enteral nutrition) could help avoid readmissions and optimize outcomes.</p>","PeriodicalId":10278,"journal":{"name":"Clinical and Translational Gastroenterology","volume":" ","pages":"e00848"},"PeriodicalIF":3.0000,"publicationDate":"2025-05-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12330361/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Translational Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14309/ctg.0000000000000848","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Hospital readmission rate is a key hospital metric and represents a substantial burden to patients and the healthcare system. Necrotizing pancreatitis (NP) patients are at high risk of unplanned readmission. The aim of this study was to determine the incidence and predictors of 30-day unplanned readmission after index hospitalization for NP.
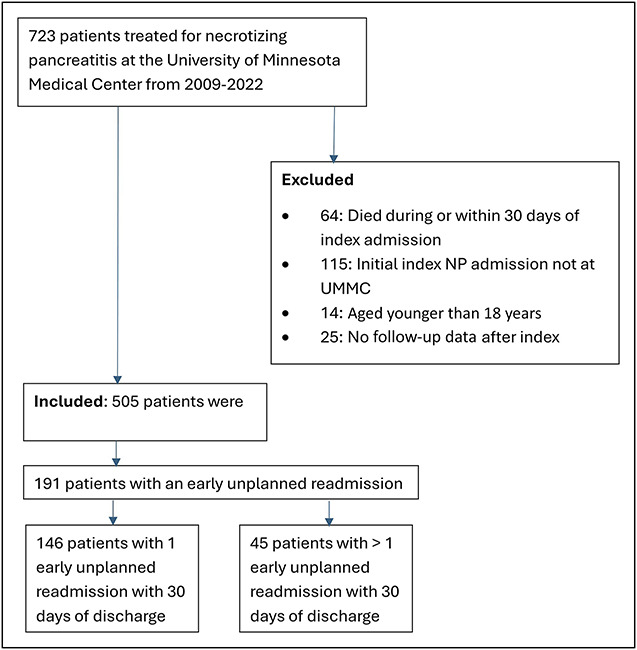
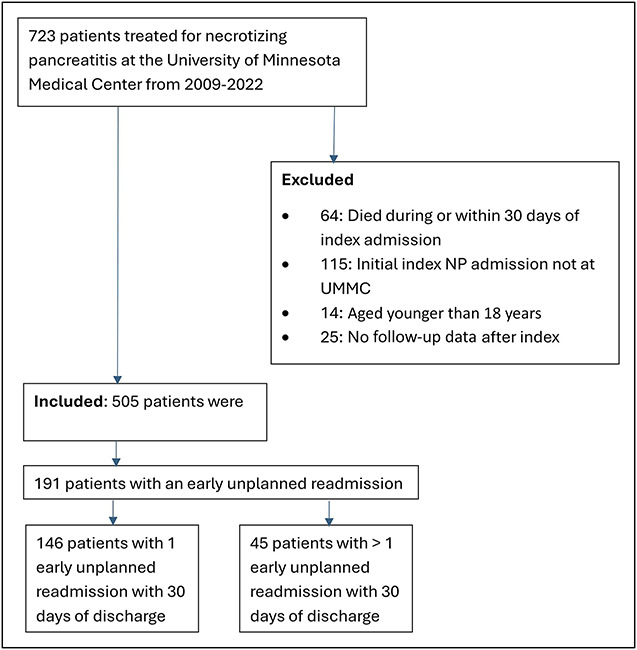
Methods: Adult NP patients who were managed at a single tertiary referral center between 2009 and 2022 were identified from a prospective database and categorized into 2 groups based on 30-day unplanned readmission after index hospitalization. Patients with no follow-up who died during index admission or within 30 days of discharge were excluded. Baseline data on admission including demographic, clinical, interventional, imaging, and discharge characteristics were compared. Multivariable analysis was completed to identify independent predictors of 30-day readmission.
Results: Among 505 patients with NP (male patients-347 [69%], median age-50 years [inter quartile range 37-63]) 191 (37.8%) had at least 1 unplanned readmission. The most common causes of readmission were abdominal pain (40%) and sepsis (27%). On multivariable analysis, independent predictors for early readmission were necrosis collection size ≥ 6 cm (adjusted odds ratio [aOR] 1.91 [1.11-3.30], P < 0.03), stay at outside hospital ≥ 14 days before transfer to tertiary center (aOR 2.89 [1.27-6.60], P < 0.01), and need for percutaneous feeding tube at the time of discharge (aOR 2.06 [1.01-4.21], P < 0.05).
Discussion: Readmission after NP is common and associated with greater mortality at 6 months. Expedited transfer to tertiary center for timely intervention, assiduous follow-up of other high-risk patients (large collections and those who need enteral nutrition) could help avoid readmissions and optimize outcomes.
期刊介绍:
Clinical and Translational Gastroenterology (CTG), published on behalf of the American College of Gastroenterology (ACG), is a peer-reviewed open access online journal dedicated to innovative clinical work in the field of gastroenterology and hepatology. CTG hopes to fulfill an unmet need for clinicians and scientists by welcoming novel cohort studies, early-phase clinical trials, qualitative and quantitative epidemiologic research, hypothesis-generating research, studies of novel mechanisms and methodologies including public health interventions, and integration of approaches across organs and disciplines. CTG also welcomes hypothesis-generating small studies, methods papers, and translational research with clear applications to human physiology or disease.
Colon and small bowel
Endoscopy and novel diagnostics
Esophagus
Functional GI disorders
Immunology of the GI tract
Microbiology of the GI tract
Inflammatory bowel disease
Pancreas and biliary tract
Liver
Pathology
Pediatrics
Preventative medicine
Nutrition/obesity
Stomach.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


