E M Strabbing, O Engin, M A J Telleman, A P Nagtegaal, E B Wolvius
{"title":"Post-traumatic and iatrogenic silent sinus syndrome: a case series.","authors":"E M Strabbing, O Engin, M A J Telleman, A P Nagtegaal, E B Wolvius","doi":"10.1007/s10006-025-01391-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Silent sinus syndrome (SSS) is a rare condition characterized by progressive maxillary sinus collapse, causing enophthalmos and hypoglobus without sinusitis symptoms. Secondary SSS arises from trauma or surgery disrupting mucociliary clearance. This study aims to analyze CT scan features, evaluate the timeline of SSS development, and identify contributing factors.</p><p><strong>Materials and methods: </strong>Patients diagnosed with secondary (post-traumatic or iatrogenic) SSS between January 2015 and January 2024 at the Erasmus Medical Center were reviewed. Characteristics from pre-SSS (T1) and post-SSS (T2) stages, management, and clinical outcomes were recorded. Data on patient demographics, symptoms, orthoptic findings, and the time interval between trauma or surgery and SSS onset were also collected.</p><p><strong>Results: </strong>Nine patients (six males and three females) met the inclusion criteria. The time from trauma or surgery to SSS onset ranged from one to thirty-six months, with a median of three months in the posttraumatic group. All patients presented with unilateral enophthalmos or hypoglobus; eight reported diplopia. Surgical management, including retrograde uncinectomy and orbital reconstruction, restored orbital anatomy and resolved symptoms.</p><p><strong>Conclusion: </strong>Secondary SSS is a rare but significant condition requiring early recognition to prevent severe cosmetic and functional complications.</p><p><strong>Clinical relevance: </strong>Secondary SSS should be considered when patients present with unexplained orbital changes following trauma or surgery. Regular follow-up is recommended, especially in patients with orbital trauma or surgery involving the inferomedial strut. Further studies are necessary to clarify risk factors associated with secondary SSS.</p><p><strong>Clinical trial number: </strong>Not applicable.</p>","PeriodicalId":520733,"journal":{"name":"Oral and maxillofacial surgery","volume":"29 1","pages":"106"},"PeriodicalIF":1.8000,"publicationDate":"2025-05-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12098178/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Oral and maxillofacial surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s10006-025-01391-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
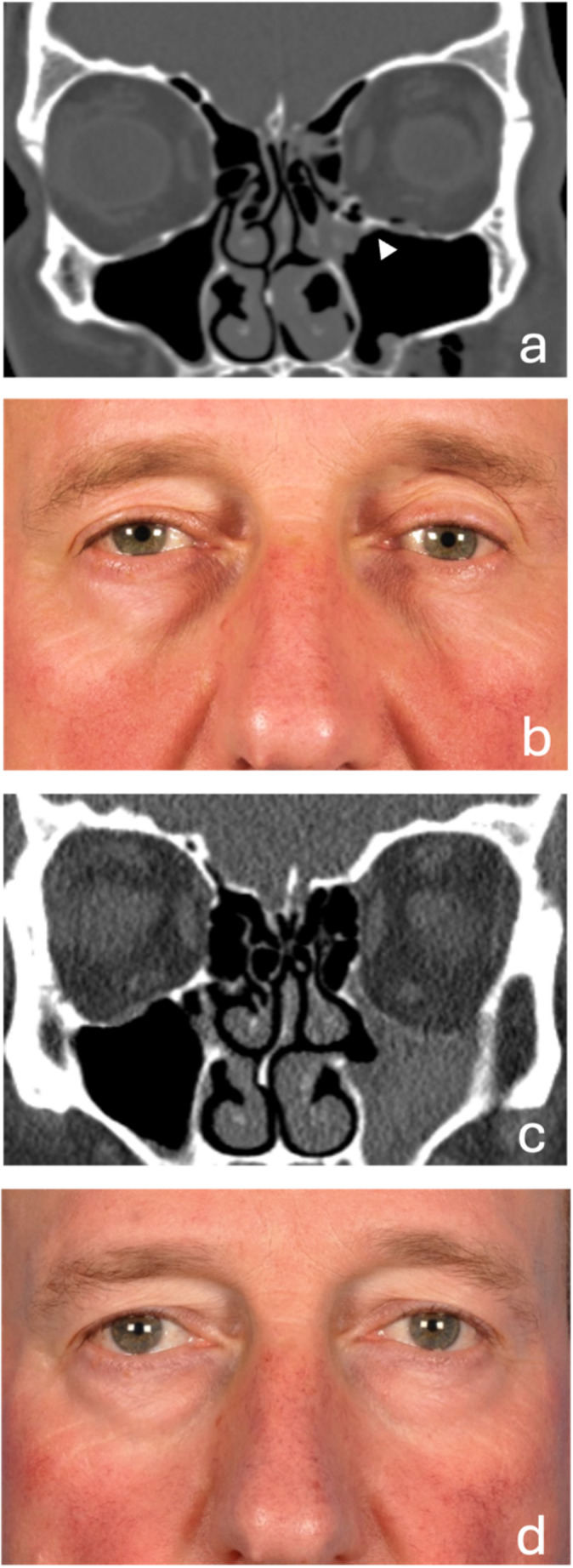
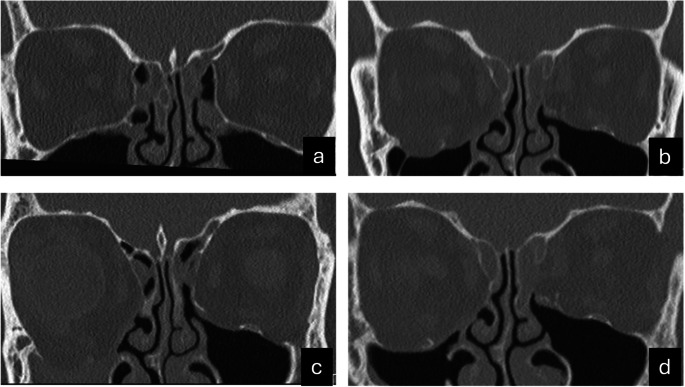
Objectives: Silent sinus syndrome (SSS) is a rare condition characterized by progressive maxillary sinus collapse, causing enophthalmos and hypoglobus without sinusitis symptoms. Secondary SSS arises from trauma or surgery disrupting mucociliary clearance. This study aims to analyze CT scan features, evaluate the timeline of SSS development, and identify contributing factors.
Materials and methods: Patients diagnosed with secondary (post-traumatic or iatrogenic) SSS between January 2015 and January 2024 at the Erasmus Medical Center were reviewed. Characteristics from pre-SSS (T1) and post-SSS (T2) stages, management, and clinical outcomes were recorded. Data on patient demographics, symptoms, orthoptic findings, and the time interval between trauma or surgery and SSS onset were also collected.
Results: Nine patients (six males and three females) met the inclusion criteria. The time from trauma or surgery to SSS onset ranged from one to thirty-six months, with a median of three months in the posttraumatic group. All patients presented with unilateral enophthalmos or hypoglobus; eight reported diplopia. Surgical management, including retrograde uncinectomy and orbital reconstruction, restored orbital anatomy and resolved symptoms.
Conclusion: Secondary SSS is a rare but significant condition requiring early recognition to prevent severe cosmetic and functional complications.
Clinical relevance: Secondary SSS should be considered when patients present with unexplained orbital changes following trauma or surgery. Regular follow-up is recommended, especially in patients with orbital trauma or surgery involving the inferomedial strut. Further studies are necessary to clarify risk factors associated with secondary SSS.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


