José-Manuel Rubio-Campal, Carlos Rodriguez Lopez, Carla Lázaro Rivera, Francisco de Asís Díaz Cortegana, Loreto Bravo Calero, Cristina Aguilera Agudo, José María Romero-Otero, José Tuñón Fernández
{"title":"Baseline left ventricular ejection fraction predicts the magnitude of improvement in patients taking sacubitril/valsartan.","authors":"José-Manuel Rubio-Campal, Carlos Rodriguez Lopez, Carla Lázaro Rivera, Francisco de Asís Díaz Cortegana, Loreto Bravo Calero, Cristina Aguilera Agudo, José María Romero-Otero, José Tuñón Fernández","doi":"10.5603/cj.104310","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sacubitril/valsartan (S/V) improve left ventricular ejection fraction (LVEF) in heart failure patients, but the magnitude of improvement may depend on baseline values.</p><p><strong>Methods: </strong>We analyzed whether baseline LVEF can predict its improvement in patients with LVEF ≤ 45% receiving S/V. Patients were divided into 4 groups (G) according to baseline LVEF (G1: ≤ 20%; G2: 21-30%; G3: 31-40%; G4: 41-45%).</p><p><strong>Results: </strong>We included 256 patients (age 73 ± 12 years; 73% male; 174 ischemic cardiomyopathy [CM], 82 nonischemic CM) and assessed LVEF at S/V initiation and at 6 and 12 months of therapy. Baseline LVEF (%) values (overall 30.9 ± 8.6) were: G1: 17.3 ± 3.3; G2: 27.5 ± 2.4; G3: 35.5 ± 2; G4: 44.4 ± 1. LVEF increased in 62% of patients, reaching 34.3 ± 10.4% and 35.5 ± 11.2% at 6 and 12 months, respectively (p < 0.001). A significantly higher absolute LVEF increase was found in Groups 3 (7.2 ± 4.3) and 4 (4.2 ± 3.05) than in Groups 1 (0.6 ± 1.5) and 2 (3.5 ± 1.5), in women (5.9 ± 4.4 vs. 4.1 ± 4.5; p < 0.001), with high S/V doses (7.4 ± 4.7 vs. 4.3 ± 4.4; p < 0.001), and in nonischemic CM (6.3 ± 4.9 vs. 3.8 ± 4.2; p < 0.001). On multivariate analysis, female sex (OR 2.18; 95% CI [1.06-4.48]; p = 0.034), high dose (OR 3.38; 95% CI [1.10-10.34]; p = 0.033), and baseline LVEF > 30% (OR 8.62; 95% CI [4.69-15.82]; p = 0.001) were significant predictors of LVEF improvement.</p><p><strong>Conclusions: </strong>LVEF improvement with S/V depends on baseline values, sex, and dose.</p>","PeriodicalId":93923,"journal":{"name":"Cardiology journal","volume":" ","pages":"270-277"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12221323/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5603/cj.104310","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/22 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Sacubitril/valsartan (S/V) improve left ventricular ejection fraction (LVEF) in heart failure patients, but the magnitude of improvement may depend on baseline values.
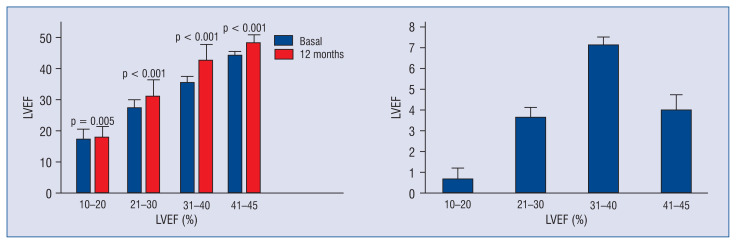
Methods: We analyzed whether baseline LVEF can predict its improvement in patients with LVEF ≤ 45% receiving S/V. Patients were divided into 4 groups (G) according to baseline LVEF (G1: ≤ 20%; G2: 21-30%; G3: 31-40%; G4: 41-45%).
Results: We included 256 patients (age 73 ± 12 years; 73% male; 174 ischemic cardiomyopathy [CM], 82 nonischemic CM) and assessed LVEF at S/V initiation and at 6 and 12 months of therapy. Baseline LVEF (%) values (overall 30.9 ± 8.6) were: G1: 17.3 ± 3.3; G2: 27.5 ± 2.4; G3: 35.5 ± 2; G4: 44.4 ± 1. LVEF increased in 62% of patients, reaching 34.3 ± 10.4% and 35.5 ± 11.2% at 6 and 12 months, respectively (p < 0.001). A significantly higher absolute LVEF increase was found in Groups 3 (7.2 ± 4.3) and 4 (4.2 ± 3.05) than in Groups 1 (0.6 ± 1.5) and 2 (3.5 ± 1.5), in women (5.9 ± 4.4 vs. 4.1 ± 4.5; p < 0.001), with high S/V doses (7.4 ± 4.7 vs. 4.3 ± 4.4; p < 0.001), and in nonischemic CM (6.3 ± 4.9 vs. 3.8 ± 4.2; p < 0.001). On multivariate analysis, female sex (OR 2.18; 95% CI [1.06-4.48]; p = 0.034), high dose (OR 3.38; 95% CI [1.10-10.34]; p = 0.033), and baseline LVEF > 30% (OR 8.62; 95% CI [4.69-15.82]; p = 0.001) were significant predictors of LVEF improvement.
Conclusions: LVEF improvement with S/V depends on baseline values, sex, and dose.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


