Mohsyn Imran Malik, Brandon Loshusan, Michael W A Chu
{"title":"Learning Curve Analysis of Minimally Invasive Mitral Valve Repair.","authors":"Mohsyn Imran Malik, Brandon Loshusan, Michael W A Chu","doi":"10.1177/15569845251337406","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Previous learning curve analyses of minimally invasive mitral valve (MV) repair have focused largely on early safety outcomes without including detailed mitral repair quality outcomes. This study investigates the learning curve of minimally invasive MV repair over a 15-year experience, focused on clinical outcomes and evidence-based technical failure endpoints.</p><p><strong>Methods: </strong>All MV repair operations were performed by a single surgeon between May 2008 and February 2023. Patient data were stratified into 3 groups of tertiles. Failure endpoints were defined as postrepair residual mitral regurgitation ≥ mild and a 30-day composite outcome. Cumulative log-likelihood curves were constructed for minimally invasive MV repair using the primary outcomes as technical failure endpoints. Control limits were determined using previous analyses of the Society of Thoracic Surgeons database.</p><p><strong>Results: </strong>A total of 362 consecutive patients across 15 years were included. Across tertiles, there was a significant trend toward shorter cross-clamp time (<i>P</i> < 0.001), cardiopulmonary bypass time (<i>P</i> < 0.001), and hospital length of stay (<i>P</i> = 0.005). Learning curve analysis demonstrated crossing of the lower threshold at ~60 patients for postrepair mitral regurgitation ≥ mild and ~85 patients for the 30-day composite outcome. The mean adjusted risk scores for both primary outcomes based on a multivariable logistic model demonstrated no significant differences across tertiles.</p><p><strong>Conclusions: </strong>The estimated number of operations to achieve optimal repair outcomes and durability is ~60 to 85 patients. These data can improve the design of surgical training competencies, beyond avoidance of complications, and instead focus the learning curve on what is necessary to achieve optimal mitral repair outcomes.</p>","PeriodicalId":13574,"journal":{"name":"Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery","volume":" ","pages":"297-303"},"PeriodicalIF":1.6000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12264299/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/15569845251337406","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/22 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Previous learning curve analyses of minimally invasive mitral valve (MV) repair have focused largely on early safety outcomes without including detailed mitral repair quality outcomes. This study investigates the learning curve of minimally invasive MV repair over a 15-year experience, focused on clinical outcomes and evidence-based technical failure endpoints.
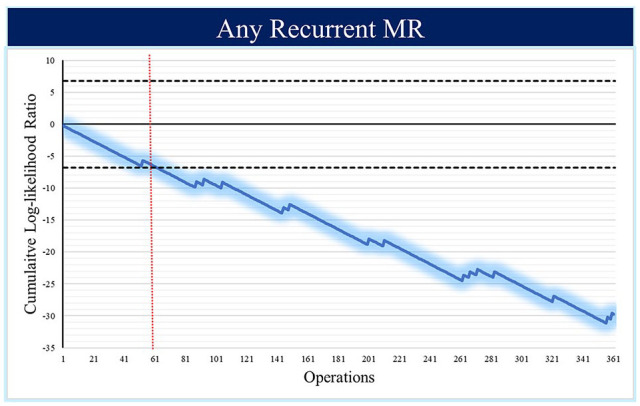
Methods: All MV repair operations were performed by a single surgeon between May 2008 and February 2023. Patient data were stratified into 3 groups of tertiles. Failure endpoints were defined as postrepair residual mitral regurgitation ≥ mild and a 30-day composite outcome. Cumulative log-likelihood curves were constructed for minimally invasive MV repair using the primary outcomes as technical failure endpoints. Control limits were determined using previous analyses of the Society of Thoracic Surgeons database.
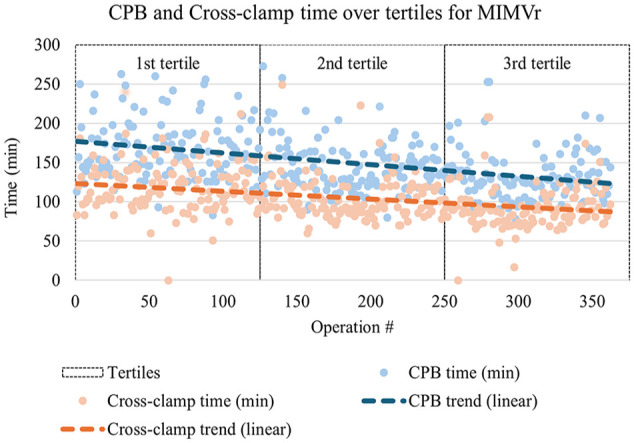
Results: A total of 362 consecutive patients across 15 years were included. Across tertiles, there was a significant trend toward shorter cross-clamp time (P < 0.001), cardiopulmonary bypass time (P < 0.001), and hospital length of stay (P = 0.005). Learning curve analysis demonstrated crossing of the lower threshold at ~60 patients for postrepair mitral regurgitation ≥ mild and ~85 patients for the 30-day composite outcome. The mean adjusted risk scores for both primary outcomes based on a multivariable logistic model demonstrated no significant differences across tertiles.
Conclusions: The estimated number of operations to achieve optimal repair outcomes and durability is ~60 to 85 patients. These data can improve the design of surgical training competencies, beyond avoidance of complications, and instead focus the learning curve on what is necessary to achieve optimal mitral repair outcomes.
期刊介绍:
Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery is the first journal whose main mission is to disseminate information specifically about advances in technology and techniques that lead to less invasive treatment of cardiothoracic and vascular disease. It delivers cutting edge original research, reviews, essays, case reports, and editorials from the pioneers and experts in the field of minimally invasive cardiothoracic and vascular disease, including biomedical engineers. Also included are papers presented at the annual ISMICS meeting. Official Journal of the International Society for Minimally Invasive Cardiothoracic Surgery

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


