Josseline Madrid, William J Young, Stefan van Duijvenboden, Michele Orini, Patricia B Munroe, Julia Ramírez, Ana Mincholé
{"title":"Unsupervised clustering of single-lead electrocardiograms associates with prevalent and incident heart failure in coronary artery disease.","authors":"Josseline Madrid, William J Young, Stefan van Duijvenboden, Michele Orini, Patricia B Munroe, Julia Ramírez, Ana Mincholé","doi":"10.1093/ehjdh/ztaf013","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Clinical consequences of coronary artery disease (CAD) are varied [e.g. atrial fibrillation (AF) and heart failure (HF)], and current risk stratification tools are ineffective. We aimed to identify clusters of individuals with CAD exhibiting unique patterns on the electrocardiogram (ECG) in an unsupervised manner and assess their association with cardiovascular risk.</p><p><strong>Methods and results: </strong>Twenty-one ECG markers were derived from single-lead median-beat ECGs of 1928 individuals with CAD without a previous diagnosis of AF, HF, or ventricular arrhythmia (VA) from the imaging study in UK Biobank (CAD-IMG-UKB). An unsupervised clustering algorithm was used to group these markers into distinct clusters. We characterized each cluster according to their demographic and ECG characteristics, as well as their prevalent and incident risk of AF, HF, and VA (4-year median follow-up). Validation and association with prevalent diagnoses were performed in an independent cohort of 1644 individuals. The model identified two clusters within the CAD-IMG-UKB cohort. Cluster 1 (<i>n</i> = 359) exhibited prolonged QRS duration and QT intervals, along with greater morphological variations in QRS and T-waves, compared with Cluster 2 (<i>n</i> = 1569). Cluster 1, relative to Cluster 2, had a significantly higher risk of incident HF [hazard ratio (HR): 2.40, 95% confidence interval (CI): 1.51-3.83], confirmed by independent validation (HR: 1.77, CI: 1.31-2.41). It also showed a higher association with prevalent HF (odds ratio: 4.10, CI: 2.02-8.29), independent of clinical risk factors.</p><p><strong>Conclusion: </strong>Our approach identified a cluster of individuals with CAD sharing ECG characteristics indicating HF risk, holding significant implications for targeted treatment and prevention enabling accessible large-scale screening.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"6 3","pages":"435-446"},"PeriodicalIF":4.4000,"publicationDate":"2025-03-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12088720/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztaf013","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
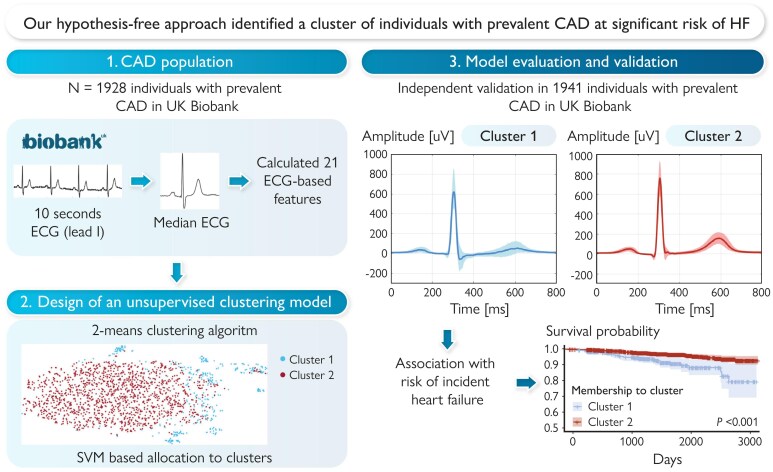
Aims: Clinical consequences of coronary artery disease (CAD) are varied [e.g. atrial fibrillation (AF) and heart failure (HF)], and current risk stratification tools are ineffective. We aimed to identify clusters of individuals with CAD exhibiting unique patterns on the electrocardiogram (ECG) in an unsupervised manner and assess their association with cardiovascular risk.
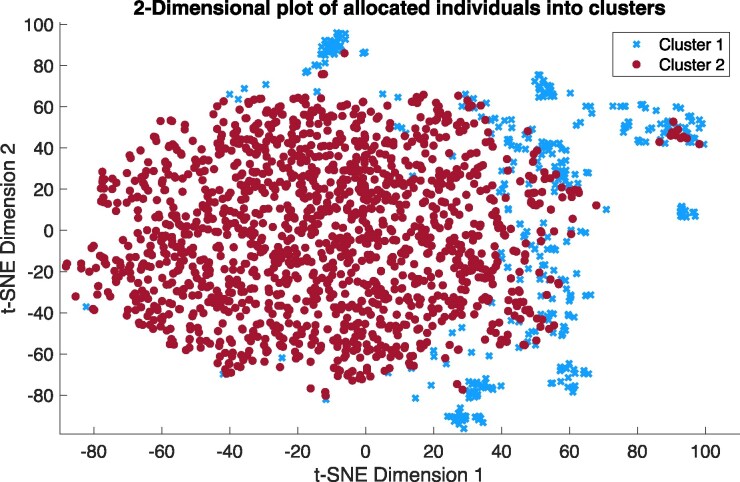
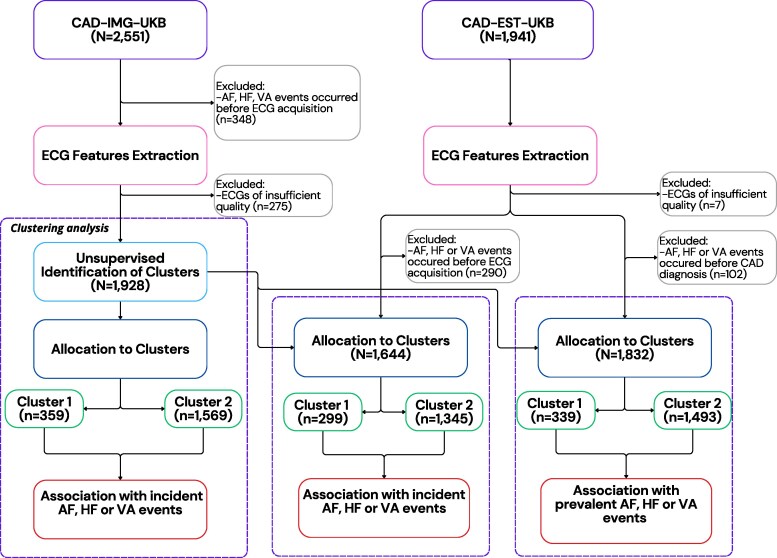
Methods and results: Twenty-one ECG markers were derived from single-lead median-beat ECGs of 1928 individuals with CAD without a previous diagnosis of AF, HF, or ventricular arrhythmia (VA) from the imaging study in UK Biobank (CAD-IMG-UKB). An unsupervised clustering algorithm was used to group these markers into distinct clusters. We characterized each cluster according to their demographic and ECG characteristics, as well as their prevalent and incident risk of AF, HF, and VA (4-year median follow-up). Validation and association with prevalent diagnoses were performed in an independent cohort of 1644 individuals. The model identified two clusters within the CAD-IMG-UKB cohort. Cluster 1 (n = 359) exhibited prolonged QRS duration and QT intervals, along with greater morphological variations in QRS and T-waves, compared with Cluster 2 (n = 1569). Cluster 1, relative to Cluster 2, had a significantly higher risk of incident HF [hazard ratio (HR): 2.40, 95% confidence interval (CI): 1.51-3.83], confirmed by independent validation (HR: 1.77, CI: 1.31-2.41). It also showed a higher association with prevalent HF (odds ratio: 4.10, CI: 2.02-8.29), independent of clinical risk factors.
Conclusion: Our approach identified a cluster of individuals with CAD sharing ECG characteristics indicating HF risk, holding significant implications for targeted treatment and prevention enabling accessible large-scale screening.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


