Feasibility, safety and patient perceptions of exercise-based cardiac telerehabilitation in a multicentre real-world setting after myocardial infarction-the remote exercise SWEDEHEART study.
Maria Bäck, Margret Leosdottir, Mattias Ekström, Kristina Hambraeus, Annica Ravn-Fischer, Sabina Borg, Madeleine Brosved, Marcus Flink, Kajsa Hedin, Charlotta Lans, Jessica Olovsson, Charlotte Urell, Birgitta Öberg, Stefan James
{"title":"Feasibility, safety and patient perceptions of exercise-based cardiac telerehabilitation in a multicentre real-world setting after myocardial infarction-the remote exercise SWEDEHEART study.","authors":"Maria Bäck, Margret Leosdottir, Mattias Ekström, Kristina Hambraeus, Annica Ravn-Fischer, Sabina Borg, Madeleine Brosved, Marcus Flink, Kajsa Hedin, Charlotta Lans, Jessica Olovsson, Charlotte Urell, Birgitta Öberg, Stefan James","doi":"10.1093/ehjdh/ztaf014","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Cardiac telerehabilitation addresses common barriers for attendance at exercise-based cardiac rehabilitation (EBCR). Pragmatic real-world studies are however lacking, limiting generalizability of available evidence. We aimed to evaluate feasibility, safety, and patient perceptions of remotely delivered EBCR in a multicentre clinical practice setting after myocardial infarction (MI).</p><p><strong>Methods and results: </strong>This study included 232 post-MI patients (63.7 years, 77.5% men) from 23 cardiac rehabilitation centres in Sweden (2020-22). Exercise was delivered twice per week for 3 months through a real-time group-based video meeting connecting a physiotherapist to patients exercising at home. Outcomes were assessed before and after remote EBCR completion and comprised assessment of physical fitness, self-reported physical activity and exercise, physical capacity, kinesiophobia, health-related quality of life (HRQoL), self-efficacy for exercise, exercise adherence, patient acceptance. Safety monitoring in terms of adverse events (AE) and serious adverse events (SAE) was recorded. A total of 67.2% of the patients attended ≥ 75% of prescribed exercise sessions. Significant improvements in physical fitness, self-reported exercise, physical capacity, kinesiophobia, and HRQoL were observed. Patients agreed that remote EBCR improved health care access (83%), was easy to use (94%) and found exercise performance and interaction acceptable (95%). Sixteen exercise-related AEs (most commonly dizziness and musculoskeletal symptoms) were registered, all of which were resolved. Two SAEs requiring hospitalization were reported, both unrelated to exercise.</p><p><strong>Conclusion: </strong>This multicentre study supports remote EBCR post-MI as feasible and safe with a high patient acceptance in a real-world setting. The clinical effectiveness needs to be confirmed in a randomized controlled trial.</p><p><strong>Trial registration number: </strong>NCT04260958.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"6 3","pages":"508-518"},"PeriodicalIF":4.4000,"publicationDate":"2025-03-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12088728/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztaf014","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Cardiac telerehabilitation addresses common barriers for attendance at exercise-based cardiac rehabilitation (EBCR). Pragmatic real-world studies are however lacking, limiting generalizability of available evidence. We aimed to evaluate feasibility, safety, and patient perceptions of remotely delivered EBCR in a multicentre clinical practice setting after myocardial infarction (MI).
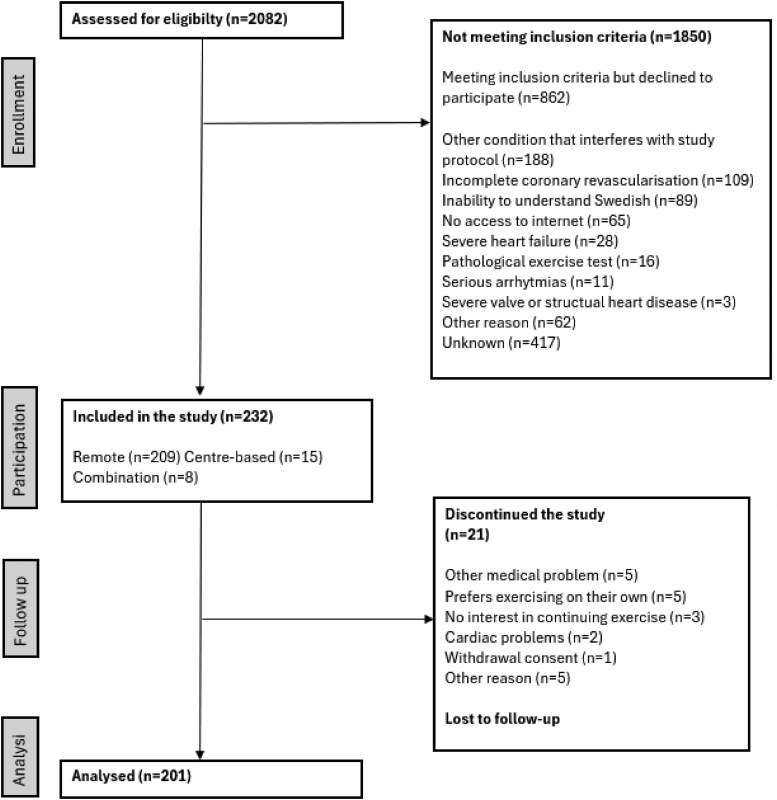
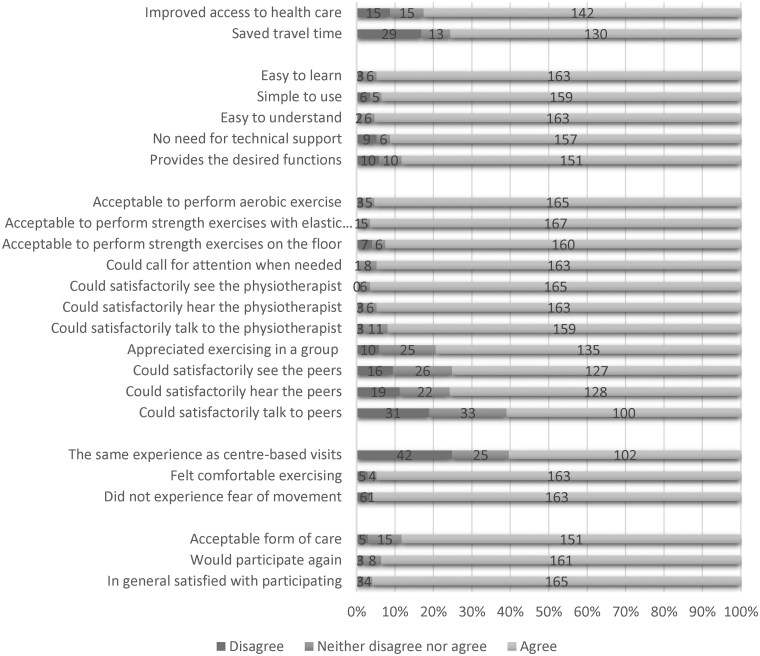
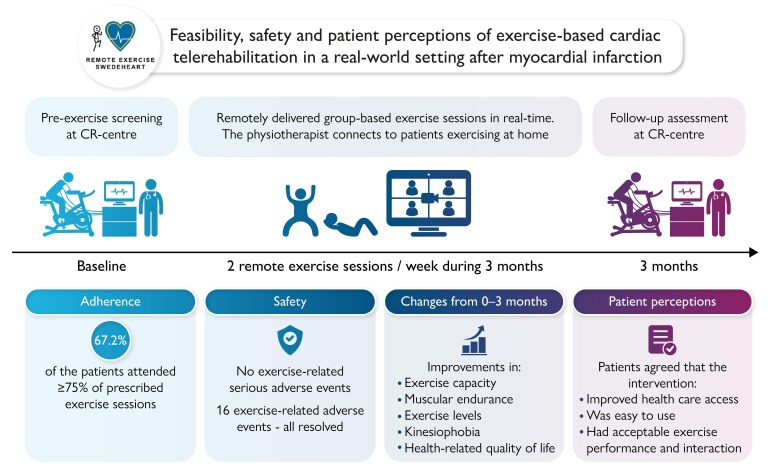
Methods and results: This study included 232 post-MI patients (63.7 years, 77.5% men) from 23 cardiac rehabilitation centres in Sweden (2020-22). Exercise was delivered twice per week for 3 months through a real-time group-based video meeting connecting a physiotherapist to patients exercising at home. Outcomes were assessed before and after remote EBCR completion and comprised assessment of physical fitness, self-reported physical activity and exercise, physical capacity, kinesiophobia, health-related quality of life (HRQoL), self-efficacy for exercise, exercise adherence, patient acceptance. Safety monitoring in terms of adverse events (AE) and serious adverse events (SAE) was recorded. A total of 67.2% of the patients attended ≥ 75% of prescribed exercise sessions. Significant improvements in physical fitness, self-reported exercise, physical capacity, kinesiophobia, and HRQoL were observed. Patients agreed that remote EBCR improved health care access (83%), was easy to use (94%) and found exercise performance and interaction acceptable (95%). Sixteen exercise-related AEs (most commonly dizziness and musculoskeletal symptoms) were registered, all of which were resolved. Two SAEs requiring hospitalization were reported, both unrelated to exercise.
Conclusion: This multicentre study supports remote EBCR post-MI as feasible and safe with a high patient acceptance in a real-world setting. The clinical effectiveness needs to be confirmed in a randomized controlled trial.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


