Ethics, orthodoxies and defensive practice: a cross-sectional survey of nurse's decision-making surrounding CPR in deceased inpatients without Do Not Resuscitate orders.
Gemma McErlean, Suzanne Bowdler, Joanne Cordina, Heidi Hui, Edwina Light, Wendy Lipworth, Susan Maitland, Eamon Merrick, Amy Montgomery, Anne Preisz, Linda Sheahan, Suzanne Sheppard-Law, George Skowronski, Cameron Stewart, Judeil Krlan Teus, Michael Watts, Sahn Zanotti, Ian Kerridge
{"title":"Ethics, orthodoxies and defensive practice: a cross-sectional survey of nurse's decision-making surrounding CPR in deceased inpatients without Do Not Resuscitate orders.","authors":"Gemma McErlean, Suzanne Bowdler, Joanne Cordina, Heidi Hui, Edwina Light, Wendy Lipworth, Susan Maitland, Eamon Merrick, Amy Montgomery, Anne Preisz, Linda Sheahan, Suzanne Sheppard-Law, George Skowronski, Cameron Stewart, Judeil Krlan Teus, Michael Watts, Sahn Zanotti, Ian Kerridge","doi":"10.1186/s12910-025-01224-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In hospital, nurses are often the first to identify patients in cardiorespiratory arrest and must decide whether to call a CODE BLUE and commence cardiopulmonary resuscitation (CPR). In Australia, there are no legal or policy obligations to commence CPR when unequivocal signs of death are present. The use of CPR where it cannot provide any benefit to a patient raises profound questions about decision-making and ethical practice. The aim of this empirical ethics study was to describe hospital-based nurses' decision-making, perspectives, and experiences of initiating CPR in hospitalised patients who have unequivocal signs of death but lack a Do-Not-Resuscitate (DNR) order.</p><p><strong>Methods: </strong>The study was a multisite cross-sectional descriptive survey conducted between October 2023-April 2024. Nurses were presented with two clinical scenarios in which patients were found to have no signs of life: Mr. D, an 84-year-old male with cancer, and Mr. G, a 35-year-old male post-motor vehicle accident. Eligible participants were all nurses working in in-patient units. Descriptive statistics, Pearson Chi-square or Fisher's exact tests, McNemar test, and binomial logistic regression were used to analyse the data.</p><p><strong>Results: </strong>531 nurses completed the survey. For Mr D, 61.5% (n = 324) would call a CODE BLUE, 24.1% (n = 127) would perform limited CPR. Only 14.4% (n = 76) would confirm death. For Mr G, 93.9% (n = 492) would call a CODE BLUE, 4.4% (n = 23) would perform limited CPR, and 1.7% (n = 9) would confirm death. The major reasons why nurses initiate a CODE BLUE were 'In the absence of an DNR order, there is no option but to begin CPR', 'I am required by hospital policy to do so', 'I am required by law to do so' and 'It is what I was trained to do'.</p><p><strong>Conclusions: </strong>Most nurses would commence CPR in patients with clear signs of death in the absence of a DNR order. This seems most likely related to ignorance or misunderstanding of law, policy and/or the misapplication or professional norms. These results raise important questions about the drivers of nurses understanding of and engagement with CPR. This highlights ethical concerns for care and treatment of patients at the end of their life and underscores the need to examine ethical practice, agency, and professionalism and supports review of policy, practices and education regarding ethical end-of-life decision making and care.</p>","PeriodicalId":55348,"journal":{"name":"BMC Medical Ethics","volume":"26 1","pages":"65"},"PeriodicalIF":3.1000,"publicationDate":"2025-05-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12090638/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Medical Ethics","FirstCategoryId":"98","ListUrlMain":"https://doi.org/10.1186/s12910-025-01224-2","RegionNum":1,"RegionCategory":"哲学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ETHICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In hospital, nurses are often the first to identify patients in cardiorespiratory arrest and must decide whether to call a CODE BLUE and commence cardiopulmonary resuscitation (CPR). In Australia, there are no legal or policy obligations to commence CPR when unequivocal signs of death are present. The use of CPR where it cannot provide any benefit to a patient raises profound questions about decision-making and ethical practice. The aim of this empirical ethics study was to describe hospital-based nurses' decision-making, perspectives, and experiences of initiating CPR in hospitalised patients who have unequivocal signs of death but lack a Do-Not-Resuscitate (DNR) order.
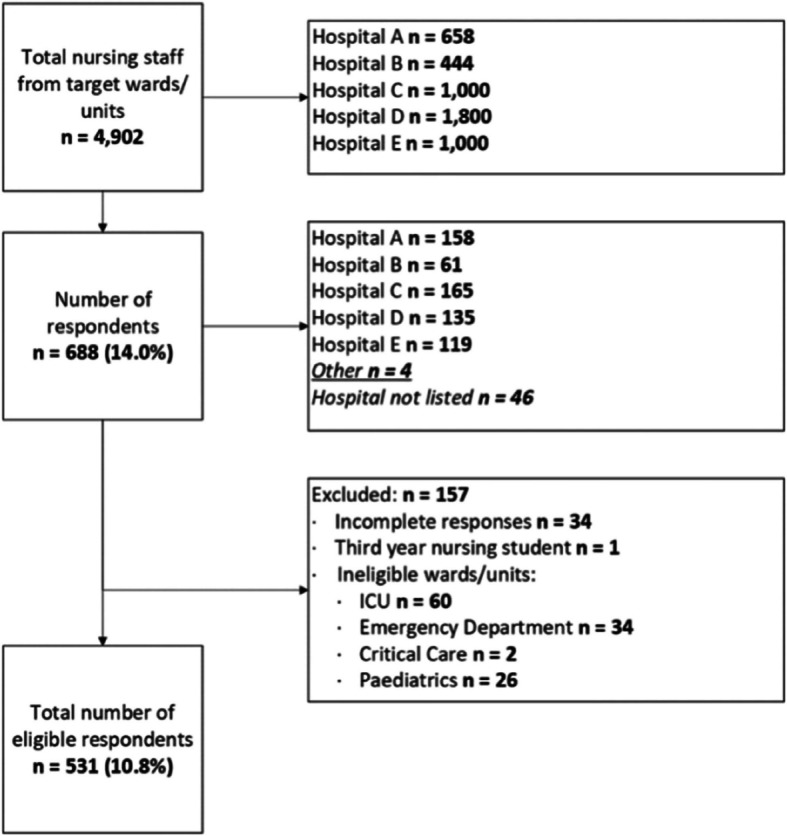
Methods: The study was a multisite cross-sectional descriptive survey conducted between October 2023-April 2024. Nurses were presented with two clinical scenarios in which patients were found to have no signs of life: Mr. D, an 84-year-old male with cancer, and Mr. G, a 35-year-old male post-motor vehicle accident. Eligible participants were all nurses working in in-patient units. Descriptive statistics, Pearson Chi-square or Fisher's exact tests, McNemar test, and binomial logistic regression were used to analyse the data.
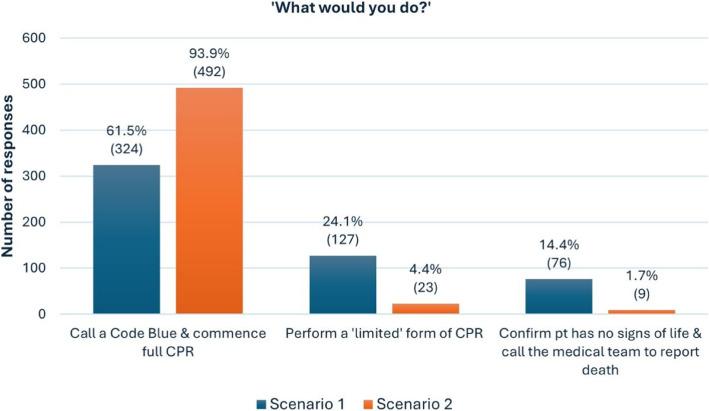
Results: 531 nurses completed the survey. For Mr D, 61.5% (n = 324) would call a CODE BLUE, 24.1% (n = 127) would perform limited CPR. Only 14.4% (n = 76) would confirm death. For Mr G, 93.9% (n = 492) would call a CODE BLUE, 4.4% (n = 23) would perform limited CPR, and 1.7% (n = 9) would confirm death. The major reasons why nurses initiate a CODE BLUE were 'In the absence of an DNR order, there is no option but to begin CPR', 'I am required by hospital policy to do so', 'I am required by law to do so' and 'It is what I was trained to do'.
Conclusions: Most nurses would commence CPR in patients with clear signs of death in the absence of a DNR order. This seems most likely related to ignorance or misunderstanding of law, policy and/or the misapplication or professional norms. These results raise important questions about the drivers of nurses understanding of and engagement with CPR. This highlights ethical concerns for care and treatment of patients at the end of their life and underscores the need to examine ethical practice, agency, and professionalism and supports review of policy, practices and education regarding ethical end-of-life decision making and care.
期刊介绍:
BMC Medical Ethics is an open access journal publishing original peer-reviewed research articles in relation to the ethical aspects of biomedical research and clinical practice, including professional choices and conduct, medical technologies, healthcare systems and health policies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


