{"title":"Intraoperative Autologous Blood Transfusion in Aortic Surgery.","authors":"Shao Feng Zhou, Akiko Tanaka, Anthony Estrera","doi":"10.1055/s-0045-1809172","DOIUrl":null,"url":null,"abstract":"<p><p>Aortic surgeries are associated with intraoperative blood loss, often requiring allogeneic blood transfusion. Therefore, blood must be viewed as a scarce resource that carries risks and benefits. Many preoperative and perioperative interventions are likely to reduce bleeding and blood transfusion. Perioperative blood conservation strategies in cardiovascular surgery are highly recommended and often necessary. In 2019, nearly 11 million units of whole blood and red blood cell units and more than 2.2 million apheresis and whole blood-derived platelet units were transfused in the United States. Intraoperative autologous blood transfusion techniques include saving red blood cells with cell saver, sparing whole blood through the acute, normovolemic hemodilution techniques, reducing hemodilution with retrograde autologous priming on cardiopulmonary bypass, and protection and reservation of coagulation factors and platelets through autologous platelet-rich plasma techniques. More than 80% of blood transfusions occur within the first 24 hours after surgical incision-with most intraoperative blood transfusions occurring between postcardiopulmonary bypass and reversed heparin before surgical closing. Intraoperative autologous blood transfusion techniques remain an important method in blood conservation strategies in aortic surgeries. Intraoperative cell savers are considered a cost-effective tool for most cardiovascular procedures or other surgeries in which substantial blood loss is expected (>500 mL).</p>","PeriodicalId":52392,"journal":{"name":"AORTA","volume":" ","pages":"153-161"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12185167/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AORTA","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0045-1809172","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/20 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
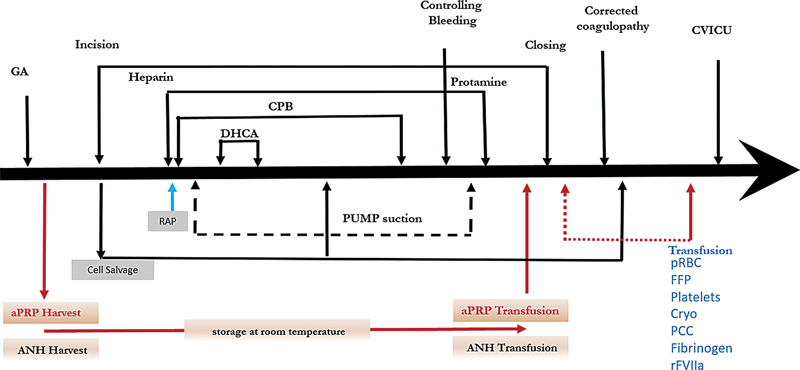
Aortic surgeries are associated with intraoperative blood loss, often requiring allogeneic blood transfusion. Therefore, blood must be viewed as a scarce resource that carries risks and benefits. Many preoperative and perioperative interventions are likely to reduce bleeding and blood transfusion. Perioperative blood conservation strategies in cardiovascular surgery are highly recommended and often necessary. In 2019, nearly 11 million units of whole blood and red blood cell units and more than 2.2 million apheresis and whole blood-derived platelet units were transfused in the United States. Intraoperative autologous blood transfusion techniques include saving red blood cells with cell saver, sparing whole blood through the acute, normovolemic hemodilution techniques, reducing hemodilution with retrograde autologous priming on cardiopulmonary bypass, and protection and reservation of coagulation factors and platelets through autologous platelet-rich plasma techniques. More than 80% of blood transfusions occur within the first 24 hours after surgical incision-with most intraoperative blood transfusions occurring between postcardiopulmonary bypass and reversed heparin before surgical closing. Intraoperative autologous blood transfusion techniques remain an important method in blood conservation strategies in aortic surgeries. Intraoperative cell savers are considered a cost-effective tool for most cardiovascular procedures or other surgeries in which substantial blood loss is expected (>500 mL).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


