Ran Svirsky, Adi Sharabi-Nov, Ron Maymon, Nadav Kugler, Moran Landau Rabbi, Richard Brown, Heidy Portillo Rodriguez, Linda Peltier, Kypros Nicolaides, Hamutal Meiri
{"title":"Prediction of Preeclampsia in Twins Using First Trimester: cffDNA Fraction, PlGF, and MAP.","authors":"Ran Svirsky, Adi Sharabi-Nov, Ron Maymon, Nadav Kugler, Moran Landau Rabbi, Richard Brown, Heidy Portillo Rodriguez, Linda Peltier, Kypros Nicolaides, Hamutal Meiri","doi":"10.1002/pd.6820","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To evaluate cell-free fetal DNA fraction (cffDNAF) as a first-trimester screening marker for preeclampsia necessitating delivery before 37 weeks' gestation in twin pregnancies alone and combined with other bio-markers.</p><p><strong>Methods: </strong>Women with two live fetuses were enrolled in the first trimester, and evaluated for cffDNAF as a first trimester preeclampsia marker alone, and with placental growth factor (PlGF), mean arterial pressure (MAP), and uterine artery pulsatility index (UtA-PI).</p><p><strong>Results: </strong>There were 20 affected women; the cffDNAF was 9.0% (IQR: 8.4%-10.3%) in the affected, compared to 14% (IQR: 11%-16%) in 163 unaffected cases (p < 0.001). The AUROC for cffDNAF was 0.73 (95% CI: 0.61-0.85, p < 0.001), PlGF had an AUROC of 0.71 (0.59-0.83, p = 0.001), MAP had AUROC of 0.61 (0.50-0.72, p = 0.053) whereas UtA-PI had AUROC of 0.54 (0.39-0.69, p > 0.05). Combining all three biomarkers yielded an AUROC of 0.89 (0.78-0.98), with a sensitivity of 81%, specificity of 90%, negative predictive value (NPV) of 97.5%, and positive predictive value (PPV) of 50.7 UtA-PI did not contribute to the AUROC.</p><p><strong>Conclusion: </strong>In twin pregnancies low first trimester cffDNAF effectively screens for preeclampsia necessitating delivery before 37 weeks' gestation, which is augmented with PlGF and MAP.</p>","PeriodicalId":20387,"journal":{"name":"Prenatal Diagnosis","volume":" ","pages":"968-978"},"PeriodicalIF":2.7000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12254431/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Prenatal Diagnosis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/pd.6820","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/21 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"GENETICS & HEREDITY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To evaluate cell-free fetal DNA fraction (cffDNAF) as a first-trimester screening marker for preeclampsia necessitating delivery before 37 weeks' gestation in twin pregnancies alone and combined with other bio-markers.
Methods: Women with two live fetuses were enrolled in the first trimester, and evaluated for cffDNAF as a first trimester preeclampsia marker alone, and with placental growth factor (PlGF), mean arterial pressure (MAP), and uterine artery pulsatility index (UtA-PI).
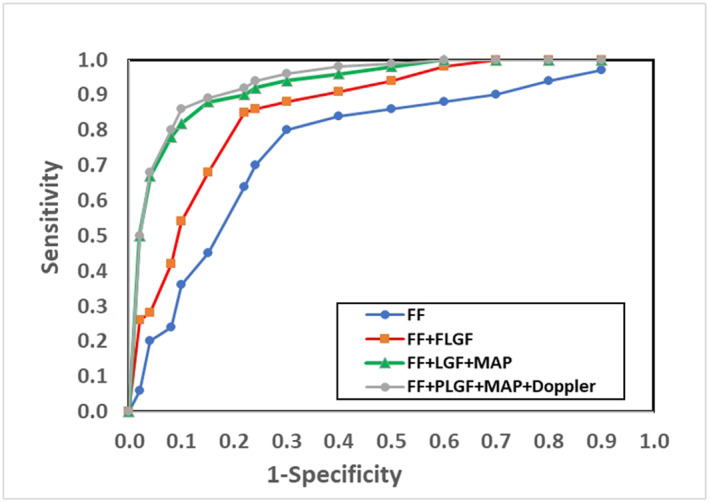
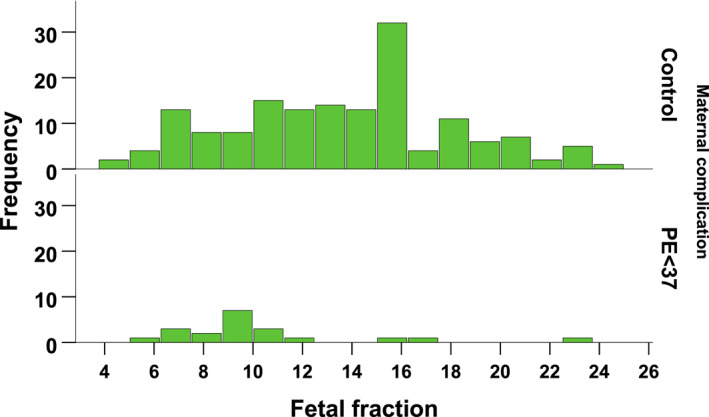
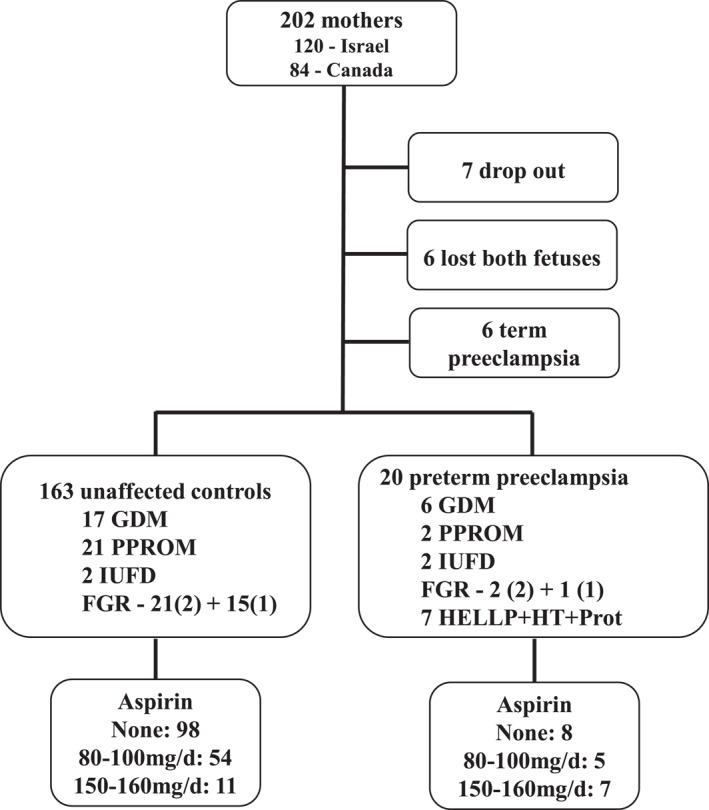
Results: There were 20 affected women; the cffDNAF was 9.0% (IQR: 8.4%-10.3%) in the affected, compared to 14% (IQR: 11%-16%) in 163 unaffected cases (p < 0.001). The AUROC for cffDNAF was 0.73 (95% CI: 0.61-0.85, p < 0.001), PlGF had an AUROC of 0.71 (0.59-0.83, p = 0.001), MAP had AUROC of 0.61 (0.50-0.72, p = 0.053) whereas UtA-PI had AUROC of 0.54 (0.39-0.69, p > 0.05). Combining all three biomarkers yielded an AUROC of 0.89 (0.78-0.98), with a sensitivity of 81%, specificity of 90%, negative predictive value (NPV) of 97.5%, and positive predictive value (PPV) of 50.7 UtA-PI did not contribute to the AUROC.
Conclusion: In twin pregnancies low first trimester cffDNAF effectively screens for preeclampsia necessitating delivery before 37 weeks' gestation, which is augmented with PlGF and MAP.
期刊介绍:
Prenatal Diagnosis welcomes submissions in all aspects of prenatal diagnosis with a particular focus on areas in which molecular biology and genetics interface with prenatal care and therapy, encompassing: all aspects of fetal imaging, including sonography and magnetic resonance imaging; prenatal cytogenetics, including molecular studies and array CGH; prenatal screening studies; fetal cells and cell-free nucleic acids in maternal blood and other fluids; preimplantation genetic diagnosis (PGD); prenatal diagnosis of single gene disorders, including metabolic disorders; fetal therapy; fetal and placental development and pathology; development and evaluation of laboratory services for prenatal diagnosis; psychosocial, legal, ethical and economic aspects of prenatal diagnosis; prenatal genetic counseling

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


