Laura A Petrauskas, Janavi Sethurathnam, Ansley J Kunnath, Rahul K Sharma, John Ceremsak, Ryan H Belcher, James D Phillips, Jay A Werkhaven, Amy S Whigham, Lyndy J Wilcox, Christopher T Wootten, Frank W Virgin, Jason S Park
{"title":"Reducing Surgery for Pediatric Posttonsillectomy Hemorrhage Using Tranexamic Acid: A Quality Improvement Initiative.","authors":"Laura A Petrauskas, Janavi Sethurathnam, Ansley J Kunnath, Rahul K Sharma, John Ceremsak, Ryan H Belcher, James D Phillips, Jay A Werkhaven, Amy S Whigham, Lyndy J Wilcox, Christopher T Wootten, Frank W Virgin, Jason S Park","doi":"10.1002/ohn.1300","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Evaluate the use of tranexamic acid (TXA) and observation as a management option for pediatric patients presenting with posttonsillectomy hemorrhage (PTH).</p><p><strong>Study design: </strong>Retrospective analysis of a prospectively implemented quality improvement initiative with a historical control comparison group.</p><p><strong>Setting: </strong>Tertiary children's hospital.</p><p><strong>Methods: </strong>Patients <18 years of age who underwent adenotonsillectomy (AT) and returned to the Emergency Department for PTH were included. Patients who were stable without large volume or active bleeding were given intravenous TXA and admitted for overnight observation. Data were compared in a before-and-after analysis: preprotocol (April 2022 to March 2023) versus postprotocol (April 2023 to March 2024). For cost-effectiveness analysis, we analyzed aggregated claims data from a commercial claims database.</p><p><strong>Results: </strong>Preprotocol 1800 adenotonsillectomies were performed, and 40 procedures were performed for control of hemorrhage (2.2 per 100 AT). Postprotocol 2356 adenotonsillectomies were performed, and 30 procedures were performed to control hemorrhage (1.3 per 100 AT) showing a significant reduction in return to the operating room (relative risk [RR] = 0.59, 95% confidence interval [CI] [0.358, 0.916], P-value .020). There were no reported adverse events attributable to TXA. An estimated 21 surgeries were avoided, and 26 additional patients were observed in the hospital during the postprotocol period, for an estimated net cost savings of $174,970.</p><p><strong>Conclusion: </strong>The implementation of a standardized TXA protocol significantly reduced the need for return to the operating room for PTH in pediatric patients, without complications and with net cost savings to the healthcare system.</p>","PeriodicalId":19707,"journal":{"name":"Otolaryngology- Head and Neck Surgery","volume":" ","pages":"745-753"},"PeriodicalIF":2.5000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12379852/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Otolaryngology- Head and Neck Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/ohn.1300","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/21 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Evaluate the use of tranexamic acid (TXA) and observation as a management option for pediatric patients presenting with posttonsillectomy hemorrhage (PTH).
Study design: Retrospective analysis of a prospectively implemented quality improvement initiative with a historical control comparison group.
Setting: Tertiary children's hospital.
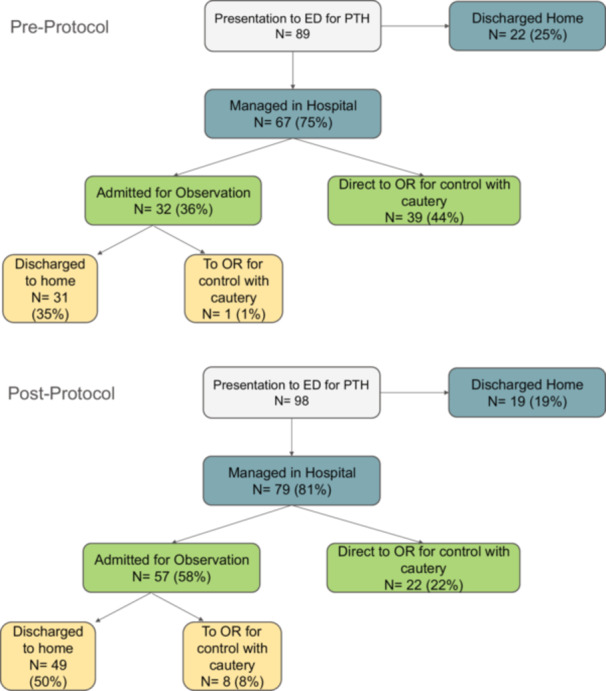
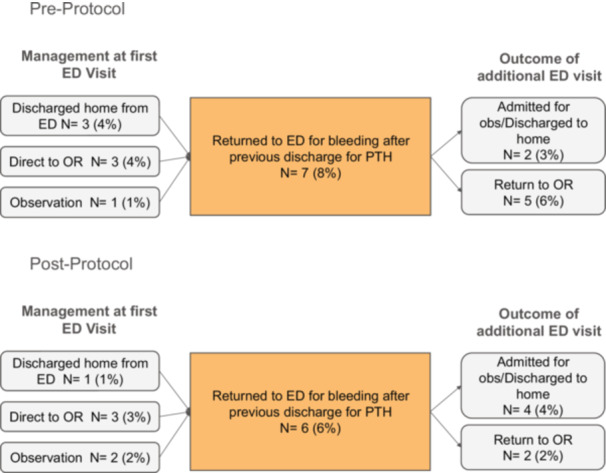
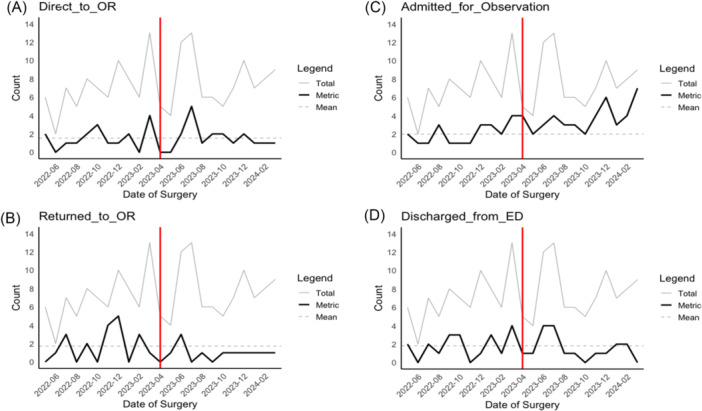
Methods: Patients <18 years of age who underwent adenotonsillectomy (AT) and returned to the Emergency Department for PTH were included. Patients who were stable without large volume or active bleeding were given intravenous TXA and admitted for overnight observation. Data were compared in a before-and-after analysis: preprotocol (April 2022 to March 2023) versus postprotocol (April 2023 to March 2024). For cost-effectiveness analysis, we analyzed aggregated claims data from a commercial claims database.
Results: Preprotocol 1800 adenotonsillectomies were performed, and 40 procedures were performed for control of hemorrhage (2.2 per 100 AT). Postprotocol 2356 adenotonsillectomies were performed, and 30 procedures were performed to control hemorrhage (1.3 per 100 AT) showing a significant reduction in return to the operating room (relative risk [RR] = 0.59, 95% confidence interval [CI] [0.358, 0.916], P-value .020). There were no reported adverse events attributable to TXA. An estimated 21 surgeries were avoided, and 26 additional patients were observed in the hospital during the postprotocol period, for an estimated net cost savings of $174,970.
Conclusion: The implementation of a standardized TXA protocol significantly reduced the need for return to the operating room for PTH in pediatric patients, without complications and with net cost savings to the healthcare system.
期刊介绍:
Otolaryngology–Head and Neck Surgery (OTO-HNS) is the official peer-reviewed publication of the American Academy of Otolaryngology–Head and Neck Surgery Foundation. The mission of Otolaryngology–Head and Neck Surgery is to publish contemporary, ethical, clinically relevant information in otolaryngology, head and neck surgery (ear, nose, throat, head, and neck disorders) that can be used by otolaryngologists, clinicians, scientists, and specialists to improve patient care and public health.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


