Sharon S Tam, Beth Williams, Rohit Kohli, Shehzad Saeed
{"title":"Standardized biopsy protocols improve adherence to eosinophilic esophagitis and celiac disease endoscopic biopsy guidelines.","authors":"Sharon S Tam, Beth Williams, Rohit Kohli, Shehzad Saeed","doi":"10.1002/jpr3.12160","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Optimal detection of eosinophilic esophagitis (EoE) and celiac disease (CeD) requires appropriate sampling of the upper gastrointestinal tract during endoscopy. However, endoscopic biopsy guidelines are poorly followed in clinical practice. A quality improvement (QI) initiative was undertaken to improve adherence to published EoE and CeD biopsy guidelines by creating standardized biopsy protocols.</p><p><strong>Methods: </strong>A biopsy form with disease-specific biopsy protocols was created and implemented. Endoscopists were initially asked to complete the form pre-procedure to indicate anticipated biopsies. After integration into the electronic health records (EHR), the form was completed by the primary treating clinician at the time endoscopy was requested. Data were collected through chart review of endoscopy and pathology reports. Statistical process control charts were used to analyze these metrics: adherence to biopsy guidelines (outcome measure), biopsy form utilization (process measure), and immediate and delayed procedural complications (balancing measures). Baseline adherence to biopsy guidelines was determined by retrospective chart review of upper endoscopies performed pre-intervention.</p><p><strong>Results: </strong>Overall adherence to biopsy guidelines improved from an average of 45% to 78.9% with our interventions. Improvement was sustained during the 2-year study period. Adherence to biopsy guidelines improved from an average of 55% to 84% for EoE and from 13.3% to 69.5% for CeD. Decreased variability in biopsy practice was noted over time. The EHR-integrated form led to consistently high utilization (>90%). Both immediate and delayed complications remained zero.</p><p><strong>Conclusions: </strong>Standardization of endoscopic biopsies using an EHR-integrated pre-procedure checklist leads to improved and sustained adherence to recommended EoE and CeD biopsy guidelines.</p>","PeriodicalId":501015,"journal":{"name":"JPGN reports","volume":"6 2","pages":"113-120"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12078035/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JPGN reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/jpr3.12160","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Optimal detection of eosinophilic esophagitis (EoE) and celiac disease (CeD) requires appropriate sampling of the upper gastrointestinal tract during endoscopy. However, endoscopic biopsy guidelines are poorly followed in clinical practice. A quality improvement (QI) initiative was undertaken to improve adherence to published EoE and CeD biopsy guidelines by creating standardized biopsy protocols.
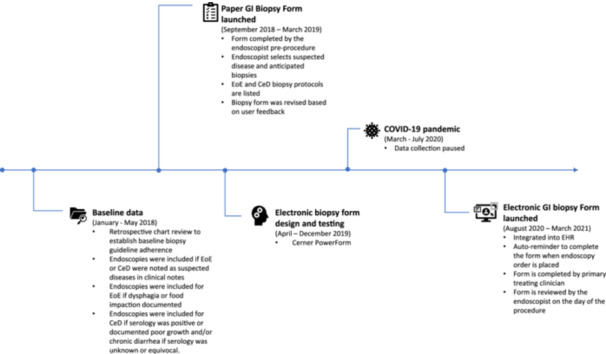
Methods: A biopsy form with disease-specific biopsy protocols was created and implemented. Endoscopists were initially asked to complete the form pre-procedure to indicate anticipated biopsies. After integration into the electronic health records (EHR), the form was completed by the primary treating clinician at the time endoscopy was requested. Data were collected through chart review of endoscopy and pathology reports. Statistical process control charts were used to analyze these metrics: adherence to biopsy guidelines (outcome measure), biopsy form utilization (process measure), and immediate and delayed procedural complications (balancing measures). Baseline adherence to biopsy guidelines was determined by retrospective chart review of upper endoscopies performed pre-intervention.
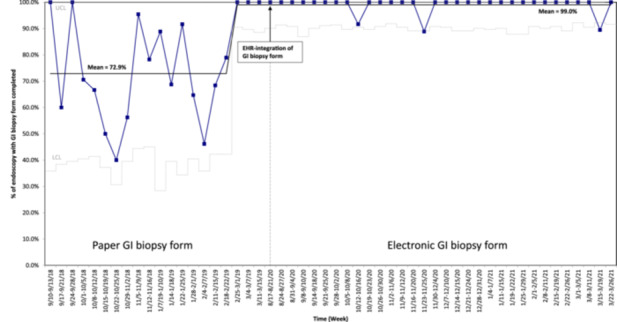
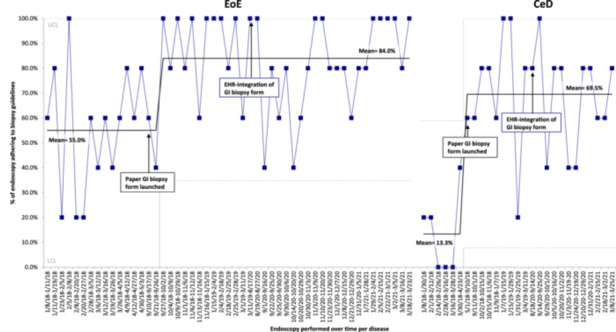
Results: Overall adherence to biopsy guidelines improved from an average of 45% to 78.9% with our interventions. Improvement was sustained during the 2-year study period. Adherence to biopsy guidelines improved from an average of 55% to 84% for EoE and from 13.3% to 69.5% for CeD. Decreased variability in biopsy practice was noted over time. The EHR-integrated form led to consistently high utilization (>90%). Both immediate and delayed complications remained zero.
Conclusions: Standardization of endoscopic biopsies using an EHR-integrated pre-procedure checklist leads to improved and sustained adherence to recommended EoE and CeD biopsy guidelines.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


