Application of the Robson classification in assessing cesarean section rates: an audit of a tertiary care hospital's gynecology department in Karachi, Pakistan.
{"title":"Application of the Robson classification in assessing cesarean section rates: an audit of a tertiary care hospital's gynecology department in Karachi, Pakistan.","authors":"Syed Muhammad Aqeel Abidi, Syeda Namayah Fatima Hussain, Shahida Abbas, Syeda Tayyaba Fatima Abidi, Sonia Haresh","doi":"10.1177/26334941251339710","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The rising rate of cesarean sections (CSs) has become a global concern due to its implications for maternal and neonatal health. The World Health Organization recommends that CS rates should not exceed 10-15% at the population level. However, many countries report rates well above this threshold.</p><p><strong>Objectives: </strong>To evaluate CS rates using the Robson Ten Group Classification System (TGCS) and identify the major contributing groups to develop targeted strategies for reducing unnecessary cesarean deliveries.</p><p><strong>Design: </strong>A retrospective clinical audit based on standardized classification and descriptive analysis.</p><p><strong>Methods: </strong>This retrospective audit was conducted using hospital delivery records from January 1st to December 31st, 2022, at the Department of Obstetrics and Gynecology, Holy Family Hospital, Karachi, Pakistan. All CSs were categorized into 10 groups using the Robson classification system. Descriptive statistics were used to determine group size, CS rate within each group, relative contribution to the overall CS rate, and absolute group contribution.</p><p><strong>Results: </strong>A total of 1464 deliveries occurred during the study period, including 507 CSs. Of these, 48.8% were elective and 51.2% were emergency CS. The major contributors to the CS rate were group 5 (51.9%), group 2 (18.5%), and group 10 (14.4%). The leading indications for cesarean delivery were previous CS (32.3%), non-progress of labor (21.15%), and cephalopelvic disproportion (16.92%).</p><p><strong>Conclusion: </strong>Targeted strategies such as promoting vaginal birth after cesarean, implementing standardized labor monitoring protocols, and strengthening antenatal counseling can help reduce unnecessary CS while maintaining maternal and neonatal safety.</p>","PeriodicalId":75219,"journal":{"name":"Therapeutic advances in reproductive health","volume":"19 ","pages":"26334941251339710"},"PeriodicalIF":1.8000,"publicationDate":"2025-05-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12081982/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic advances in reproductive health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26334941251339710","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The rising rate of cesarean sections (CSs) has become a global concern due to its implications for maternal and neonatal health. The World Health Organization recommends that CS rates should not exceed 10-15% at the population level. However, many countries report rates well above this threshold.
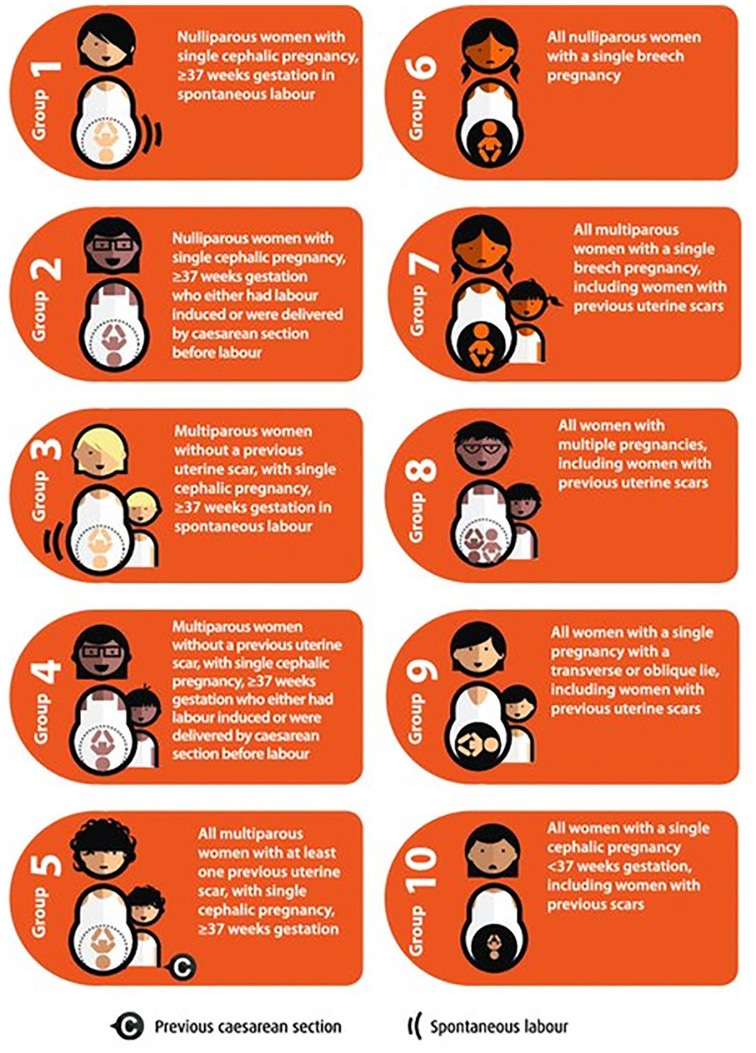
Objectives: To evaluate CS rates using the Robson Ten Group Classification System (TGCS) and identify the major contributing groups to develop targeted strategies for reducing unnecessary cesarean deliveries.
Design: A retrospective clinical audit based on standardized classification and descriptive analysis.
Methods: This retrospective audit was conducted using hospital delivery records from January 1st to December 31st, 2022, at the Department of Obstetrics and Gynecology, Holy Family Hospital, Karachi, Pakistan. All CSs were categorized into 10 groups using the Robson classification system. Descriptive statistics were used to determine group size, CS rate within each group, relative contribution to the overall CS rate, and absolute group contribution.
Results: A total of 1464 deliveries occurred during the study period, including 507 CSs. Of these, 48.8% were elective and 51.2% were emergency CS. The major contributors to the CS rate were group 5 (51.9%), group 2 (18.5%), and group 10 (14.4%). The leading indications for cesarean delivery were previous CS (32.3%), non-progress of labor (21.15%), and cephalopelvic disproportion (16.92%).
Conclusion: Targeted strategies such as promoting vaginal birth after cesarean, implementing standardized labor monitoring protocols, and strengthening antenatal counseling can help reduce unnecessary CS while maintaining maternal and neonatal safety.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


