{"title":"Developing an integrated depression and tuberculosis care pathway using a co-design approach in a low-resource setting.","authors":"Olamide Todowede, Zara Nisar, Saima Afaq, Sushama Kanan, Aliya Ayub, Rumana Huque, Akhtar Hussain, Mudasser Shehzad, Najma Siddiqi","doi":"10.1186/s13033-025-00670-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Evidence suggests the use of a participatory approach for the improvement of TB care, however, there is limited evidence on how integrated depression screening and care could be delivered with TB services. Thus, this study co-designed an integrated care pathway for depression case finding and treatment in TB services, that can be delivered by non-mental health specialists within a low resourced settings.</p><p><strong>Methods: </strong>We conducted a total of 10 'co-design' workshops with people with TB, carers, tuberculosis and mental health healthcare providers between June and August 2021 in Dhaka, Bangladesh and Peshawar, Pakistan. We adapted the 'Hasso Plattner Institute of Design at Stanford University' for our codesign process. Information gathered during the workshop, through recordings and contemporaneous notes taking, was collated, and analysed to develop the integrated care pathways and materials for impmenting the carepathway.</p><p><strong>Results: </strong>We co-designed and developed a culturally adaptable care pathway that integrates depression screening into tuberculosis (TB) care, working closely with people affected by TB and healthcare workers in primary, secondary, and tertiary care settings in Bangladesh and Pakistan. We used PHQ-9 only to identify and screen for depression among people with TB in Bangladesh, whereas both PHQ-2 and PHQ-9 were used for depression screening among the Pakistani population. A trained paramedic or laboratory technologist (Bangladesh) and DOTS Facilitator (Pakistan), working within the TB facilities were identified and agreed to deliver the integrated depression screening services.</p><p><strong>Conclusion: </strong>Stakeholders valued the opportunity to jointly design a care pathway. Iterative and coordinated working with these stakeholders enabled the researchers to understand better, explore and refine the co-design process. This approach assisted in mobilising knowledge about depression and integrating screening for depression within the existing usual TB care pathway, using the lived experience of people with TB and health workers' expertise.</p>","PeriodicalId":47752,"journal":{"name":"International Journal of Mental Health Systems","volume":"19 1","pages":"15"},"PeriodicalIF":3.8000,"publicationDate":"2025-05-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12084970/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Mental Health Systems","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13033-025-00670-0","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PSYCHIATRY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Evidence suggests the use of a participatory approach for the improvement of TB care, however, there is limited evidence on how integrated depression screening and care could be delivered with TB services. Thus, this study co-designed an integrated care pathway for depression case finding and treatment in TB services, that can be delivered by non-mental health specialists within a low resourced settings.
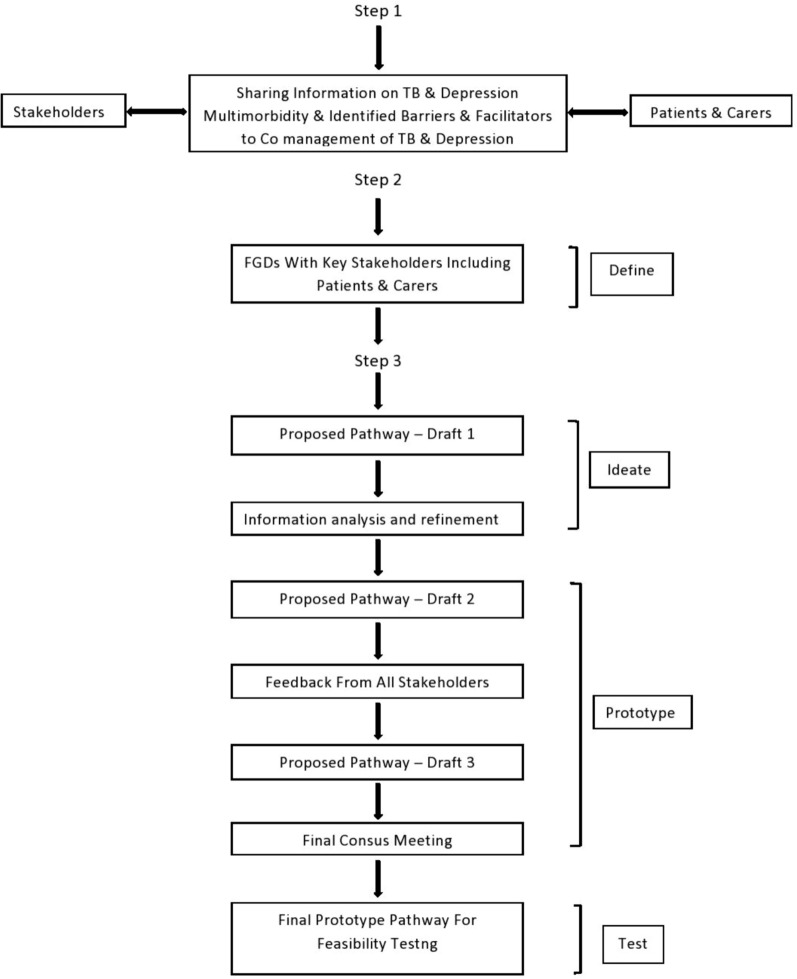
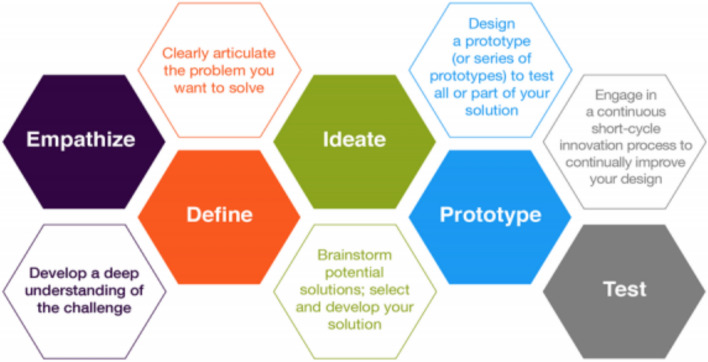
Methods: We conducted a total of 10 'co-design' workshops with people with TB, carers, tuberculosis and mental health healthcare providers between June and August 2021 in Dhaka, Bangladesh and Peshawar, Pakistan. We adapted the 'Hasso Plattner Institute of Design at Stanford University' for our codesign process. Information gathered during the workshop, through recordings and contemporaneous notes taking, was collated, and analysed to develop the integrated care pathways and materials for impmenting the carepathway.
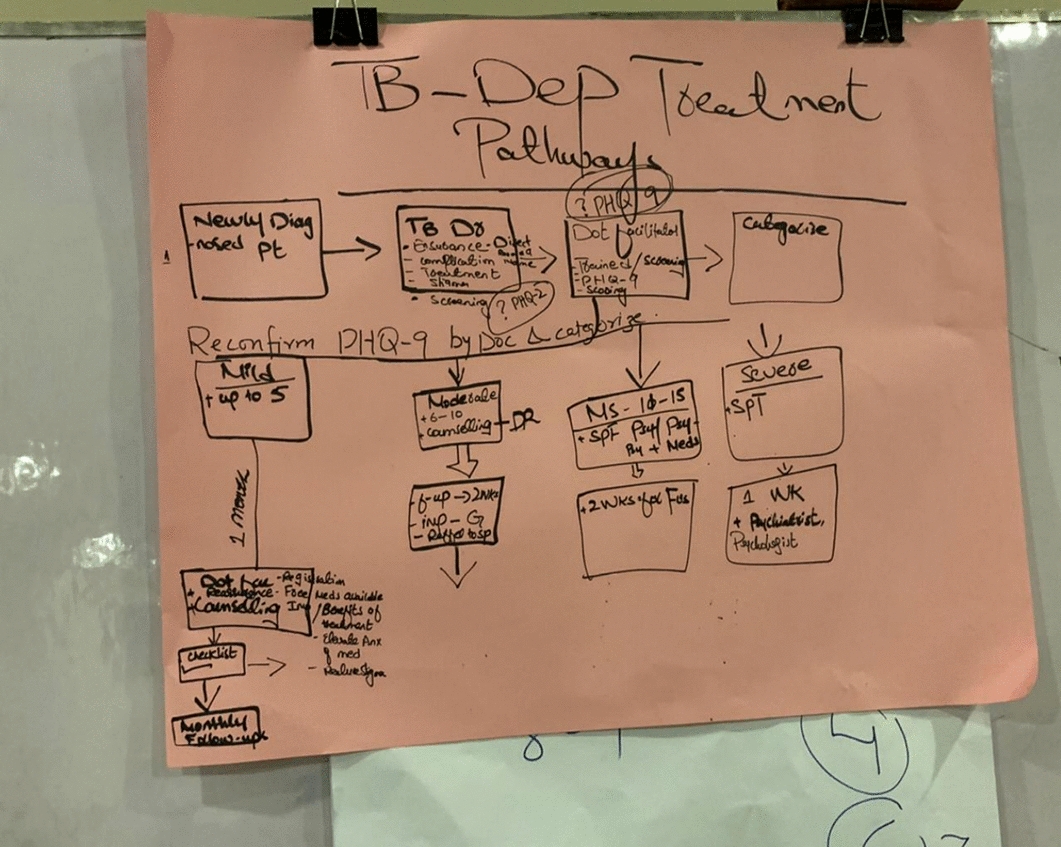
Results: We co-designed and developed a culturally adaptable care pathway that integrates depression screening into tuberculosis (TB) care, working closely with people affected by TB and healthcare workers in primary, secondary, and tertiary care settings in Bangladesh and Pakistan. We used PHQ-9 only to identify and screen for depression among people with TB in Bangladesh, whereas both PHQ-2 and PHQ-9 were used for depression screening among the Pakistani population. A trained paramedic or laboratory technologist (Bangladesh) and DOTS Facilitator (Pakistan), working within the TB facilities were identified and agreed to deliver the integrated depression screening services.
Conclusion: Stakeholders valued the opportunity to jointly design a care pathway. Iterative and coordinated working with these stakeholders enabled the researchers to understand better, explore and refine the co-design process. This approach assisted in mobilising knowledge about depression and integrating screening for depression within the existing usual TB care pathway, using the lived experience of people with TB and health workers' expertise.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


