Sara Dionne, Hillary Akana, Chris Curran, Sean Van Slyck
{"title":"Evaluation of Discrepant Infectious Disease Results in Deceased Organ Donors: Insights From a Retrospective Analysis of Post-Policy Testing.","authors":"Sara Dionne, Hillary Akana, Chris Curran, Sean Van Slyck","doi":"10.1111/tid.70055","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In 2021, a new policy was implemented by the Organ Procurement Transplant Network requiring Organ Procurement Organizations to draw a repeat blood sample for deceased organ donors if donation had not proceeded within 96-h after the initial blood sample for screening was obtained. We performed an analysis of over 2600 deceased donor test results, comparing initial results to repeated blood draw results for human immunodeficiency virus, Hepatitis B virus, and Hepatitis C virus serology and nucleic acid test (NAT) tests. This study reviews result discrepancies and explores investigations behind peculiar results.</p><p><strong>Methods: </strong>Infectious disease results from deceased organ donors were analyzed retrospectively for this study. Donor specimens were collected throughout the United States and tested at eleven laboratories. Food & Drug Administration-approved donor screening tests were used to determine donor eligibility.</p><p><strong>Results: </strong>There was a 1.69% discrepancy rate comparing results from repeat blood draw specimens to original specimen results. Of these discrepancies, 0.75% of the donors had results (enzyme-linked immunoassay and/or NAT) that changed from non-reactive to reactive. 0.68% of donors had results that changed from reactive to non-reactive. 0.26% of results changed from Ultrio repeatedly reactive, non-discriminated to either non-reactive or reactive.</p><p><strong>Conclusion: </strong>This study represents that there is more than a 1% chance that discrepant results will be obtained. Despite the low incidence of discrepancies, these rare occurrences can complicate clinical decision-making, requiring case-by-case assessments. We present several cases in which variability in results can make clinical decisions complex with limited information and the inability to perform timely confirmatory testing using tests not required by Organ Procurement Transplant Network regulations.</p>","PeriodicalId":23318,"journal":{"name":"Transplant Infectious Disease","volume":" ","pages":"e70055"},"PeriodicalIF":2.6000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12416474/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplant Infectious Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/tid.70055","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/19 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
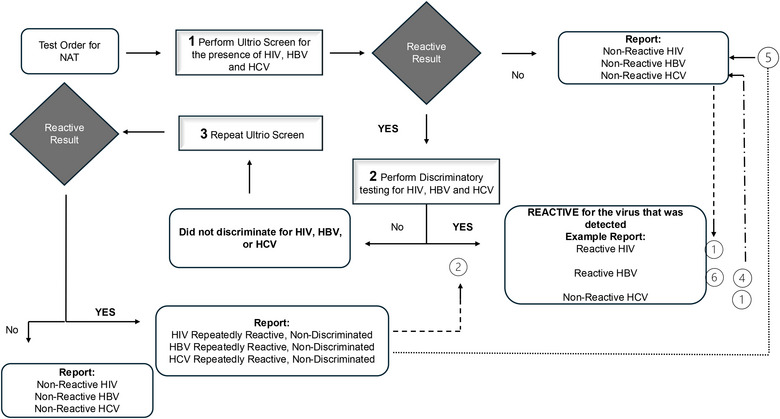
Background: In 2021, a new policy was implemented by the Organ Procurement Transplant Network requiring Organ Procurement Organizations to draw a repeat blood sample for deceased organ donors if donation had not proceeded within 96-h after the initial blood sample for screening was obtained. We performed an analysis of over 2600 deceased donor test results, comparing initial results to repeated blood draw results for human immunodeficiency virus, Hepatitis B virus, and Hepatitis C virus serology and nucleic acid test (NAT) tests. This study reviews result discrepancies and explores investigations behind peculiar results.
Methods: Infectious disease results from deceased organ donors were analyzed retrospectively for this study. Donor specimens were collected throughout the United States and tested at eleven laboratories. Food & Drug Administration-approved donor screening tests were used to determine donor eligibility.
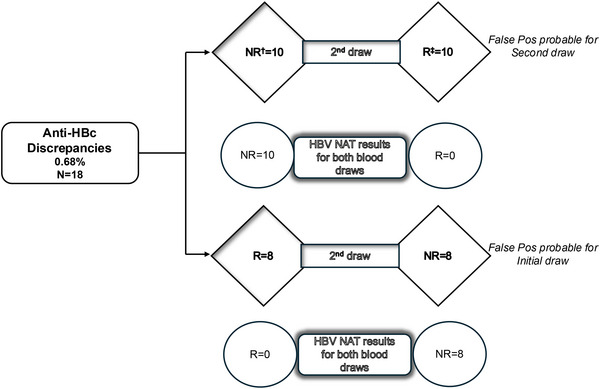
Results: There was a 1.69% discrepancy rate comparing results from repeat blood draw specimens to original specimen results. Of these discrepancies, 0.75% of the donors had results (enzyme-linked immunoassay and/or NAT) that changed from non-reactive to reactive. 0.68% of donors had results that changed from reactive to non-reactive. 0.26% of results changed from Ultrio repeatedly reactive, non-discriminated to either non-reactive or reactive.
Conclusion: This study represents that there is more than a 1% chance that discrepant results will be obtained. Despite the low incidence of discrepancies, these rare occurrences can complicate clinical decision-making, requiring case-by-case assessments. We present several cases in which variability in results can make clinical decisions complex with limited information and the inability to perform timely confirmatory testing using tests not required by Organ Procurement Transplant Network regulations.
期刊介绍:
Transplant Infectious Disease has been established as a forum for presenting the most current information on the prevention and treatment of infection complicating organ and bone marrow transplantation. The point of view of the journal is that infection and allograft rejection (or graft-versus-host disease) are closely intertwined, and that advances in one area will have immediate consequences on the other. The interaction of the transplant recipient with potential microbial invaders, the impact of immunosuppressive strategies on this interaction, and the effects of cytokines, growth factors, and chemokines liberated during the course of infections, rejection, or graft-versus-host disease are central to the interests and mission of this journal.
Transplant Infectious Disease is aimed at disseminating the latest information relevant to the infectious disease complications of transplantation to clinicians and scientists involved in bone marrow, kidney, liver, heart, lung, intestinal, and pancreatic transplantation. The infectious disease consequences and concerns regarding innovative transplant strategies, from novel immunosuppressive agents to xenotransplantation, are very much a concern of this journal. In addition, this journal feels a particular responsibility to inform primary care practitioners in the community, who increasingly are sharing the responsibility for the care of these patients, of the special considerations regarding the prevention and treatment of infection in transplant recipients. As exemplified by the international editorial board, articles are sought throughout the world that address both general issues and those of a more restricted geographic import.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


