{"title":"Predictors of difficulty in robotic splenic flexure mobilization during rectal cancer surgery.","authors":"Yusuke Yamaoka, Akio Shiomi, Hiroyasu Kagawa, Hitoshi Hino, Shoichi Manabe, Yusuke Tanaka, Shunsuke Kasai, Tetsushi Ishiguro, Akifumi Notsu","doi":"10.1007/s00384-025-04916-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>In surgery for rectal cancer, splenic flexure mobilization is sometimes necessary to ensure a tension-free colorectal anastomosis with adequate blood supply. Splenic flexure mobilization is regarded as a challenging and risky maneuver, but there are no clear indicators of its difficulty in rectal cancer surgery. This study evaluated the impact of clinical and anatomical factors, including splenic flexure height measured qualitatively on the basis of vertebral level using computed tomography, on the difficulty of splenic flexure mobilization during rectal cancer surgery.</p><p><strong>Methods: </strong>The enrolled patients underwent robotic splenic flexure mobilization during rectal surgery for primary rectal cancer at Shizuoka Cancer Center in Japan between December 2011 and March 2022. All patients were scheduled to undergo splenic flexure mobilization preoperatively, and all procedures were carried out following a standardized approach. Linear regression analysis was conducted to determine the clinical and anatomical factors significantly influencing the operative time of the abdominal phase, which is defined as the duration from lymph node dissection around the inferior mesenteric artery to the mobilization of the sigmoid and descending colon, including the splenic flexure.</p><p><strong>Results: </strong>The median operative time for the abdominal phase was 88 min (range, 39-179 min). Univariate analysis revealed that the following variables were significantly correlated with a prolonged abdominal phase: higher body mass index, larger visceral fat area, and higher splenic flexure. In a multiple linear regression analysis, only higher splenic flexure remained significantly associated with a longer abdominal phase (p < 0.01).</p><p><strong>Conclusions: </strong>Splenic flexure height measured on the basis of vertebral level using computed tomography may be useful for predicting the difficulty of robotic splenic flexure mobilization in surgery for rectal cancer.</p>","PeriodicalId":13789,"journal":{"name":"International Journal of Colorectal Disease","volume":"40 1","pages":"122"},"PeriodicalIF":2.3000,"publicationDate":"2025-05-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12085353/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Colorectal Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00384-025-04916-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
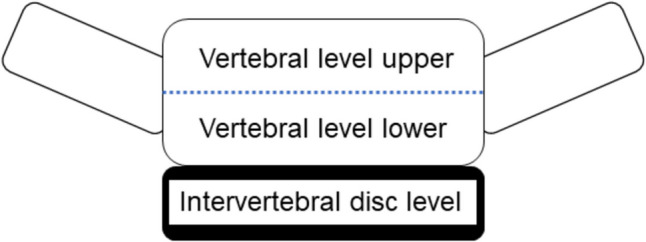
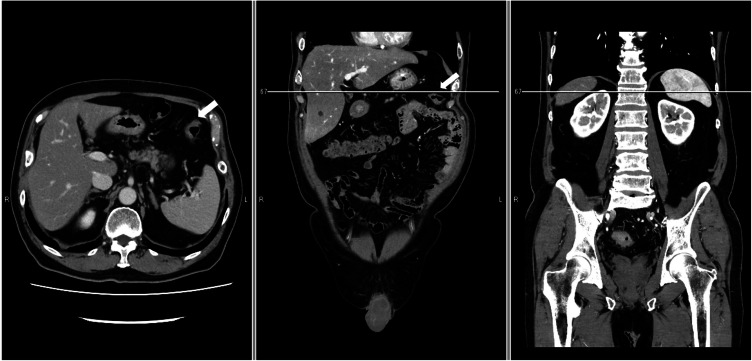
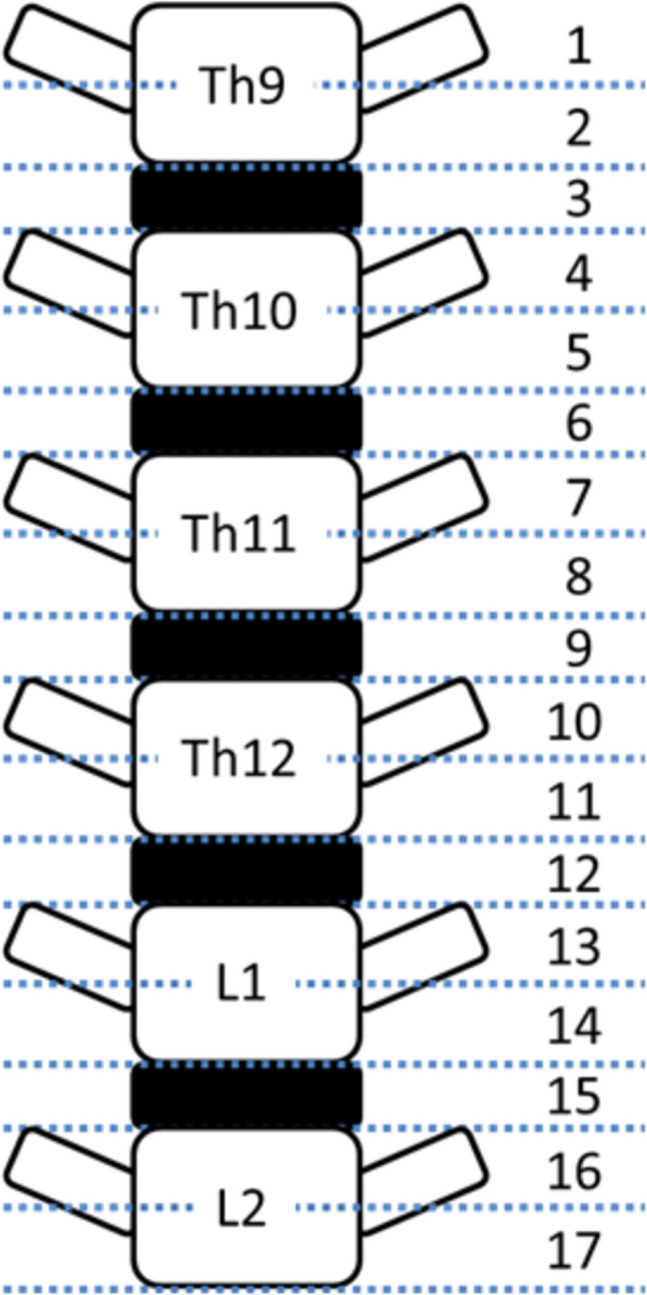
Purpose: In surgery for rectal cancer, splenic flexure mobilization is sometimes necessary to ensure a tension-free colorectal anastomosis with adequate blood supply. Splenic flexure mobilization is regarded as a challenging and risky maneuver, but there are no clear indicators of its difficulty in rectal cancer surgery. This study evaluated the impact of clinical and anatomical factors, including splenic flexure height measured qualitatively on the basis of vertebral level using computed tomography, on the difficulty of splenic flexure mobilization during rectal cancer surgery.
Methods: The enrolled patients underwent robotic splenic flexure mobilization during rectal surgery for primary rectal cancer at Shizuoka Cancer Center in Japan between December 2011 and March 2022. All patients were scheduled to undergo splenic flexure mobilization preoperatively, and all procedures were carried out following a standardized approach. Linear regression analysis was conducted to determine the clinical and anatomical factors significantly influencing the operative time of the abdominal phase, which is defined as the duration from lymph node dissection around the inferior mesenteric artery to the mobilization of the sigmoid and descending colon, including the splenic flexure.
Results: The median operative time for the abdominal phase was 88 min (range, 39-179 min). Univariate analysis revealed that the following variables were significantly correlated with a prolonged abdominal phase: higher body mass index, larger visceral fat area, and higher splenic flexure. In a multiple linear regression analysis, only higher splenic flexure remained significantly associated with a longer abdominal phase (p < 0.01).
Conclusions: Splenic flexure height measured on the basis of vertebral level using computed tomography may be useful for predicting the difficulty of robotic splenic flexure mobilization in surgery for rectal cancer.
期刊介绍:
The International Journal of Colorectal Disease, Clinical and Molecular Gastroenterology and Surgery aims to publish novel and state-of-the-art papers which deal with the physiology and pathophysiology of diseases involving the entire gastrointestinal tract. In addition to original research articles, the following categories will be included: reviews (usually commissioned but may also be submitted), case reports, letters to the editor, and protocols on clinical studies.
The journal offers its readers an interdisciplinary forum for clinical science and molecular research related to gastrointestinal disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


