Natalia A Pożarowszczyk, Iwona Kurkowska-Jastrzębska, Iwona M Sarzyńska-Długosz, Maciej Nowak, Michał Karliński
{"title":"The real-life reliability of the modified Rankin scale used in a stroke unit and a rehabilitation ward.","authors":"Natalia A Pożarowszczyk, Iwona Kurkowska-Jastrzębska, Iwona M Sarzyńska-Długosz, Maciej Nowak, Michał Karliński","doi":"10.5114/ppn.2025.149879","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The modified Rankin scale (mRS) is the gold standard for measuring stroke-related disability in clinical trials and everyday practice. However, inter-observer variability is a source of bias that may undermine the reliability of retrospective studies. It may also depend on clinical backgrounds of different assessing physician. Our aim was to prospectively assess real-life consistency between stroke unit physicians (SUPs) and physical and rehabilitation medicine physicians (PRMPs) using mRS in patients transferred directly from a stroke unit (SU) to a rehabilitation ward (RW).</p><p><strong>Methods: </strong>We enrolled 48 consented stroke patients transferred within the same hospital from SU to RW. Patients were scored in mRS by a SUP and a PRMP at the day of transfer as a standard of care. The reference mRS score (REF) was obtained by a single- blinded stroke physician using the Rankin Focused Assessment form to guide an interview.</p><p><strong>Results: </strong>An mRS score was reported for all patients admitted to the RW and 33 patients discharged from the SU. The overall agreement was 75.8% between the assessments of SUPs and PRMPs (κ = 0.58), 72.7% between SUPs and the REF (κ = 0.55) and 70.0% between PRMPs and the REF (κ = 0.49). A similar agreement was observed for PRMPs and the REF in the sensitivity cohort of 48 patients (66.7%; κ = 0.46). Patients with the REF mRS of 2 (<i>n</i> = 6) were often scored as 3 both by SUPs (4/6) and PRMPs (5/6). In patients with the REF mRS of 3 or 4 there was no clear tendency towards overrating disability.</p><p><strong>Conclusions: </strong>The reliability of mRS scoring in everyday practice is modest and does not seem to depend on clinical background of assessing physician.</p>","PeriodicalId":74481,"journal":{"name":"Postepy psychiatrii neurologii","volume":"34 1","pages":"19-25"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12076130/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Postepy psychiatrii neurologii","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/ppn.2025.149879","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/30 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: The modified Rankin scale (mRS) is the gold standard for measuring stroke-related disability in clinical trials and everyday practice. However, inter-observer variability is a source of bias that may undermine the reliability of retrospective studies. It may also depend on clinical backgrounds of different assessing physician. Our aim was to prospectively assess real-life consistency between stroke unit physicians (SUPs) and physical and rehabilitation medicine physicians (PRMPs) using mRS in patients transferred directly from a stroke unit (SU) to a rehabilitation ward (RW).
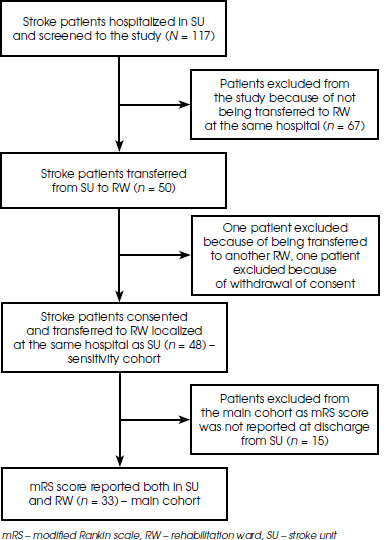
Methods: We enrolled 48 consented stroke patients transferred within the same hospital from SU to RW. Patients were scored in mRS by a SUP and a PRMP at the day of transfer as a standard of care. The reference mRS score (REF) was obtained by a single- blinded stroke physician using the Rankin Focused Assessment form to guide an interview.
Results: An mRS score was reported for all patients admitted to the RW and 33 patients discharged from the SU. The overall agreement was 75.8% between the assessments of SUPs and PRMPs (κ = 0.58), 72.7% between SUPs and the REF (κ = 0.55) and 70.0% between PRMPs and the REF (κ = 0.49). A similar agreement was observed for PRMPs and the REF in the sensitivity cohort of 48 patients (66.7%; κ = 0.46). Patients with the REF mRS of 2 (n = 6) were often scored as 3 both by SUPs (4/6) and PRMPs (5/6). In patients with the REF mRS of 3 or 4 there was no clear tendency towards overrating disability.
Conclusions: The reliability of mRS scoring in everyday practice is modest and does not seem to depend on clinical background of assessing physician.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


