Ahmad Alkhawam, Lina Okar, Ibrahem Hanafi, Peyton Murin, Ali Ibrahim, Juman Isstaif, Eman Khashaneh, Rami Z Morsi, Tareq Kass-Hout
{"title":"Rivaroxaban Versus Warfarin for the Treatment of Cerebral Venous Thrombosis (RWCVT): A Randomized Controlled Trial in Resource-Limited Setting.","authors":"Ahmad Alkhawam, Lina Okar, Ibrahem Hanafi, Peyton Murin, Ali Ibrahim, Juman Isstaif, Eman Khashaneh, Rami Z Morsi, Tareq Kass-Hout","doi":"10.1155/srat/8893742","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Cerebral venous thrombosis (CVT) is a rare but potentially debilitating form of stroke. Current management guidelines recommend a course of low molecular weight heparin (LMWH) followed by an oral vitamin K antagonist. However, there is an emerging body of evidence to support the use of direct oral anticoagulant (DOAC) medications. Here, we assess the efficacy of rivaroxaban compared to the standard of care in a resource-limited setting. <b>Methods:</b> The study was designed as a Phase III, prospective, parallel, open-label, randomized controlled trial conducted in three sites in Syria. Seventy-one participants met inclusion criteria and were randomized 1:1 to receive either rivaroxaban or warfarin following initial bridging with LMWH for 3.5-12 days. The primary outcome was functional improvement determined by the Barthel Index. Secondary outcomes were adverse events during follow-up, including CVT recurrence, thrombotic events, intracranial pressure (ICP) requiring shunt placement, extra and intracranial bleeding, neurological deficit, and all-cause mortality. <b>Results:</b> Barthel Index scores did not differ between the study cohorts at 1-, 2-, 3-, 4-, 5-, or 6-month follow-up. Secondary analysis yielded no difference in rates of adverse effects or return of CVT. Two patients in the warfarin group developed major extracranial bleeds (uterine bleeding); however, there were no other extracranial or intracranial bleeds or thrombotic events reported. Rates of all-cause mortality and all assessed adverse effects were similar between the groups. <b>Conclusion:</b> We offer a prospective, parallel randomized controlled trial that suggests rivaroxaban may have comparable safety and efficacy when compared to warfarin for the treatment of CVT. Importantly, we offer the first randomized control trial of oral anticoagulants for the treatment of CVT in a resource-limited setting, providing support for the evolving literature and suggesting the safety and efficacy of oral anticoagulants in the management of CVT. <b>Trial Registration:</b> ClinicalTrials.gov identifier: NCT04569279.</p>","PeriodicalId":22054,"journal":{"name":"Stroke Research and Treatment","volume":"2025 ","pages":"8893742"},"PeriodicalIF":1.6000,"publicationDate":"2025-05-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12081145/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Stroke Research and Treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/srat/8893742","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
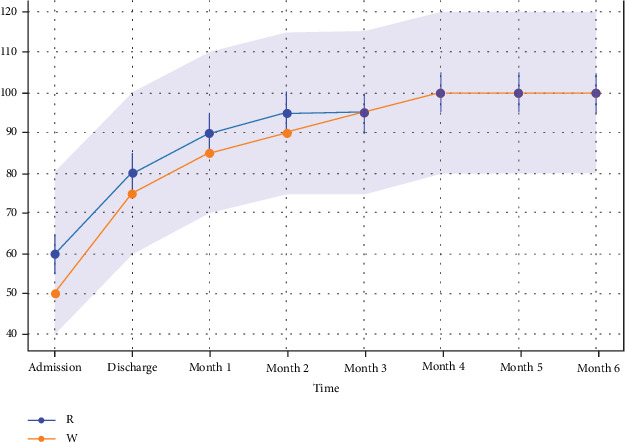
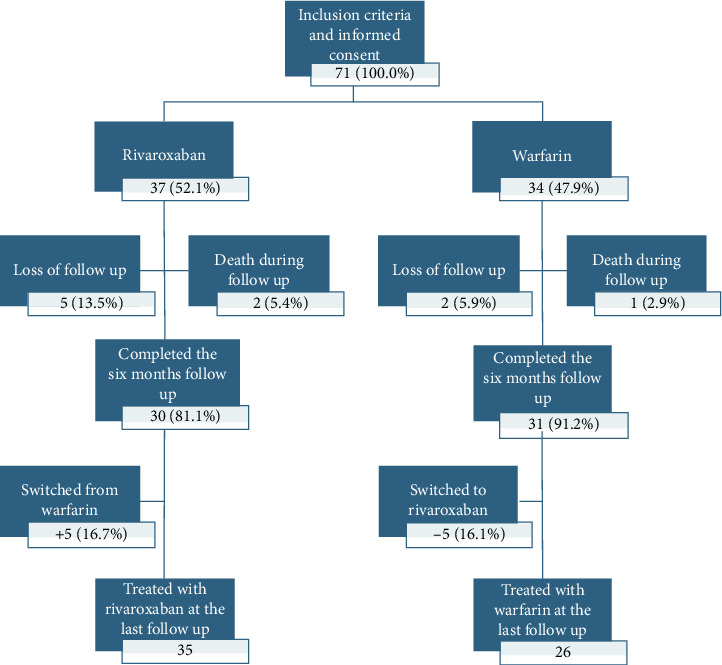
Background: Cerebral venous thrombosis (CVT) is a rare but potentially debilitating form of stroke. Current management guidelines recommend a course of low molecular weight heparin (LMWH) followed by an oral vitamin K antagonist. However, there is an emerging body of evidence to support the use of direct oral anticoagulant (DOAC) medications. Here, we assess the efficacy of rivaroxaban compared to the standard of care in a resource-limited setting. Methods: The study was designed as a Phase III, prospective, parallel, open-label, randomized controlled trial conducted in three sites in Syria. Seventy-one participants met inclusion criteria and were randomized 1:1 to receive either rivaroxaban or warfarin following initial bridging with LMWH for 3.5-12 days. The primary outcome was functional improvement determined by the Barthel Index. Secondary outcomes were adverse events during follow-up, including CVT recurrence, thrombotic events, intracranial pressure (ICP) requiring shunt placement, extra and intracranial bleeding, neurological deficit, and all-cause mortality. Results: Barthel Index scores did not differ between the study cohorts at 1-, 2-, 3-, 4-, 5-, or 6-month follow-up. Secondary analysis yielded no difference in rates of adverse effects or return of CVT. Two patients in the warfarin group developed major extracranial bleeds (uterine bleeding); however, there were no other extracranial or intracranial bleeds or thrombotic events reported. Rates of all-cause mortality and all assessed adverse effects were similar between the groups. Conclusion: We offer a prospective, parallel randomized controlled trial that suggests rivaroxaban may have comparable safety and efficacy when compared to warfarin for the treatment of CVT. Importantly, we offer the first randomized control trial of oral anticoagulants for the treatment of CVT in a resource-limited setting, providing support for the evolving literature and suggesting the safety and efficacy of oral anticoagulants in the management of CVT. Trial Registration: ClinicalTrials.gov identifier: NCT04569279.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


