Volkan Semiz, Hasan Oguz Cetinayak, Barbaros Aydin, Cenk Umay, Fadime Can
{"title":"Surgery to chemoradiotherapy time may not impact outcomes in glioblastoma patients treated with modern techniques: a single-institution study.","authors":"Volkan Semiz, Hasan Oguz Cetinayak, Barbaros Aydin, Cenk Umay, Fadime Can","doi":"10.2478/raon-2025-0031","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Surgery followed by chemoradiotherapy (CRT) with temozolomide is the standard treatment for glioblastoma patients. But, the time between surgery and CRT is still a controversial issue. This study investigated the impact of delay in CRT after surgery on overall (OS) and progression-free survival (PFS).</p><p><strong>Patients and methods: </strong>Patients aged ≥ 18 years with IDH-wild type glioblastoma, who received 60 Gy concomitant CRT with temozolomide were included in the study. Exclusion criteria include patients who underwent biopsy only, had an Eastern Cooperative Oncology Group (ECOG) performance status > 1, or presented with multicentric tumors. The interval between surgery and CRT was categorized according to 42 days, and delays after this point were defined as delayed treatment initiation. Statistical analyses included Kaplan-Meier survival analysis and Cox regression models.</p><p><strong>Results: </strong>The median OS for the regular and delayed groups was 18 and 19 months, and the PFS was 11.8 and 14.6 months, respectively. Delayed patients showed better PFS, but no statistically significant difference was found between the groups in terms of OS and PFS (p = 0.149, p = 0.076). In multivariate analysis, ECOG performance score 1 and subtotal resection were associated with poor prognosis for both OS and PFS (for OS p = 0.031, p < 0.001; for PFS p = 0.038, p = 0.029). When the time from surgery to CRT was analyzed according to the extent of surgery, no significant difference was observed in OS and PFS (p = 0.068, P = 0.057).</p><p><strong>Conclusions: </strong>Our findings showed that delays of more than 42 days in adjuvant CRT did not affect OS or PFS. However, further studies are needed to evaluate the effects of delayed adjuvant therapy in patients with subtotal resection.</p>","PeriodicalId":21034,"journal":{"name":"Radiology and Oncology","volume":" ","pages":"244-251"},"PeriodicalIF":2.2000,"publicationDate":"2025-05-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12288945/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiology and Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2478/raon-2025-0031","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Surgery followed by chemoradiotherapy (CRT) with temozolomide is the standard treatment for glioblastoma patients. But, the time between surgery and CRT is still a controversial issue. This study investigated the impact of delay in CRT after surgery on overall (OS) and progression-free survival (PFS).
Patients and methods: Patients aged ≥ 18 years with IDH-wild type glioblastoma, who received 60 Gy concomitant CRT with temozolomide were included in the study. Exclusion criteria include patients who underwent biopsy only, had an Eastern Cooperative Oncology Group (ECOG) performance status > 1, or presented with multicentric tumors. The interval between surgery and CRT was categorized according to 42 days, and delays after this point were defined as delayed treatment initiation. Statistical analyses included Kaplan-Meier survival analysis and Cox regression models.
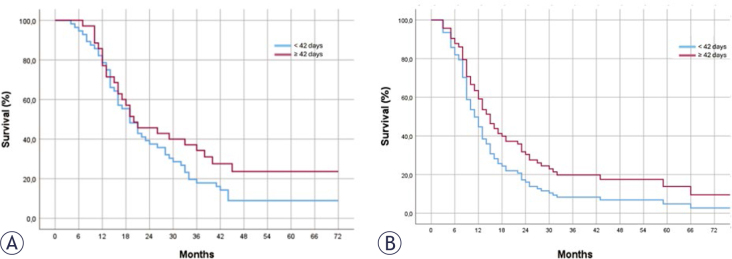
Results: The median OS for the regular and delayed groups was 18 and 19 months, and the PFS was 11.8 and 14.6 months, respectively. Delayed patients showed better PFS, but no statistically significant difference was found between the groups in terms of OS and PFS (p = 0.149, p = 0.076). In multivariate analysis, ECOG performance score 1 and subtotal resection were associated with poor prognosis for both OS and PFS (for OS p = 0.031, p < 0.001; for PFS p = 0.038, p = 0.029). When the time from surgery to CRT was analyzed according to the extent of surgery, no significant difference was observed in OS and PFS (p = 0.068, P = 0.057).
Conclusions: Our findings showed that delays of more than 42 days in adjuvant CRT did not affect OS or PFS. However, further studies are needed to evaluate the effects of delayed adjuvant therapy in patients with subtotal resection.
背景:手术加替莫唑胺放化疗是胶质母细胞瘤患者的标准治疗方法。但是,手术和CRT之间的时间仍然是一个有争议的问题。本研究探讨了术后延迟CRT对总生存率(OS)和无进展生存率(PFS)的影响。患者和方法:年龄≥18岁的idh -野生型胶质母细胞瘤患者,接受60 Gy CRT联合替莫唑胺治疗。排除标准包括仅行活检的患者,东部肿瘤合作组(ECOG)表现状态为bbb1或表现为多中心肿瘤的患者。手术与CRT的间隔时间按42天划分,超过42天的延迟定义为延迟开始治疗。统计分析包括Kaplan-Meier生存分析和Cox回归模型。结果:常规组和延迟组的中位OS分别为18和19个月,PFS分别为11.8和14.6个月。延迟患者的PFS较好,但组间OS和PFS差异无统计学意义(p = 0.149, p = 0.076)。在多因素分析中,ECOG表现评分1分和次全切除与OS和PFS的不良预后相关(OS p = 0.031, p < 0.001;PFS p = 0.038, p = 0.029)。根据手术程度分析手术至CRT时间,OS与PFS无显著差异(p = 0.068, p = 0.057)。结论:我们的研究结果显示,辅助CRT延迟超过42天不会影响OS或PFS。然而,需要进一步的研究来评估延迟辅助治疗对次全切除术患者的影响。
期刊介绍:
Radiology and Oncology is a multidisciplinary journal devoted to the publishing original and high quality scientific papers and review articles, pertinent to diagnostic and interventional radiology, computerized tomography, magnetic resonance, ultrasound, nuclear medicine, radiotherapy, clinical and experimental oncology, radiobiology, medical physics and radiation protection. Therefore, the scope of the journal is to cover beside radiology the diagnostic and therapeutic aspects in oncology, which distinguishes it from other journals in the field.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


