Yu-Hsiang Wu, Elizabeth Stangl, Kjersten Branscome, Jacob Oleson, Todd Ricketts
{"title":"Hearing Aid Service Models, Technology, and Patient Outcomes: A Randomized Clinical Trial.","authors":"Yu-Hsiang Wu, Elizabeth Stangl, Kjersten Branscome, Jacob Oleson, Todd Ricketts","doi":"10.1001/jamaoto.2025.1008","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>The poor affordability of hearing aids (HAs) limits their adoption. To justify higher costs, HAs fitted by audiologists (AUD service model) and high-end HAs should deliver better outcomes than over-the-counter (OTC) service models and low-end HAs.</p><p><strong>Objective: </strong>To determine the effect of HA service models (AUD, OTC, and a hybrid OTC+ model) and technology levels (high end and low end) on patient outcomes.</p><p><strong>Design, setting, and participants: </strong>This randomized clinical trial was conducted at the University of Iowa and Vanderbilt University Medical Center in research laboratories from February 2019 to December 2023 and included adults older than 55 years with mild to moderate hearing loss and no previous HA experience who were randomly assigned to 1 of 6 parallel groups, representing factorial combinations of 3 service models and 2 technology levels. The data were analyzed between January 2024 and March 2024.</p><p><strong>Interventions: </strong>The trial included 3 service models: AUD, in which audiologists fitted prescription HAs following best practices; OTC+, in which audiologists provided limited services for OTC HAs; and OTC, in which participants independently used OTC HAs. OTC HAs were simulated using prescription HAs. Two models of prescription HAs were used throughout the trial: a high-end HA with advanced features and a low-end HA.</p><p><strong>Main outcomes and measures: </strong>The primary outcome measure was the Glasgow Hearing Aid Benefit Profile (GHABP), which was administered using ecological momentary assessment (EMA). EMA-GHABP was conducted preintervention and throughout the seventh week postintervention.</p><p><strong>Results: </strong>A total of 245 participants completed the study (121 women [49.4%]; mean [SD] age, 67.7 [8.1] years). After controlling for preintervention scores, the postintervention EMA-GHABP global score (ranging from 1 to 5) for AUD was significantly higher (indicating better outcomes) than for OTC+ and OTC by 0.33 points (95% CI, 0.14-0.52) and 0.32 points (95% CI, 0.13-0.51), respectively. The difference between OTC+ and OTC was not significant (0.02 points, 95% CI, -0.21 to 0.18). Nevertheless, EMA-GHABP global scores for OTC+ and OTC were close to 4 points, indicating positive outcomes. The effect of technology level and interaction between service model and technology level were not significant.</p><p><strong>Conclusions and relevance: </strong>The trial results suggest that while OTC+ and OTC were effective, they did not achieve the same outcomes as AUD. As high-end and low-end HAs yielded similar outcomes, support for the higher cost of high-end HAs was not identified for individuals with mild to moderate hearing loss.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov Identifier: NCT03579563.</p>","PeriodicalId":14632,"journal":{"name":"JAMA otolaryngology-- head & neck surgery","volume":" ","pages":"684-692"},"PeriodicalIF":5.6000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12082484/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA otolaryngology-- head & neck surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1001/jamaoto.2025.1008","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: The poor affordability of hearing aids (HAs) limits their adoption. To justify higher costs, HAs fitted by audiologists (AUD service model) and high-end HAs should deliver better outcomes than over-the-counter (OTC) service models and low-end HAs.
Objective: To determine the effect of HA service models (AUD, OTC, and a hybrid OTC+ model) and technology levels (high end and low end) on patient outcomes.
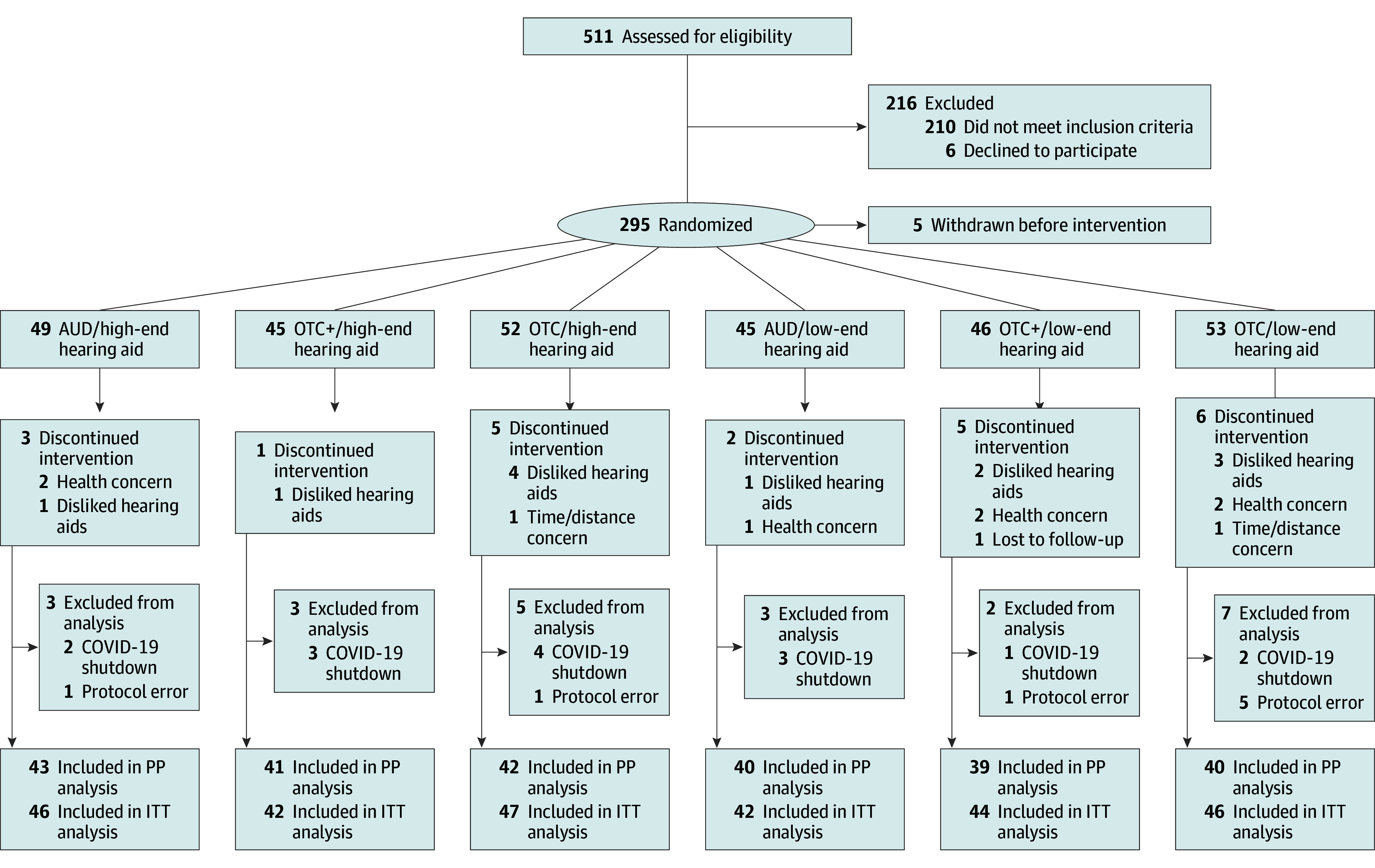
Design, setting, and participants: This randomized clinical trial was conducted at the University of Iowa and Vanderbilt University Medical Center in research laboratories from February 2019 to December 2023 and included adults older than 55 years with mild to moderate hearing loss and no previous HA experience who were randomly assigned to 1 of 6 parallel groups, representing factorial combinations of 3 service models and 2 technology levels. The data were analyzed between January 2024 and March 2024.
Interventions: The trial included 3 service models: AUD, in which audiologists fitted prescription HAs following best practices; OTC+, in which audiologists provided limited services for OTC HAs; and OTC, in which participants independently used OTC HAs. OTC HAs were simulated using prescription HAs. Two models of prescription HAs were used throughout the trial: a high-end HA with advanced features and a low-end HA.
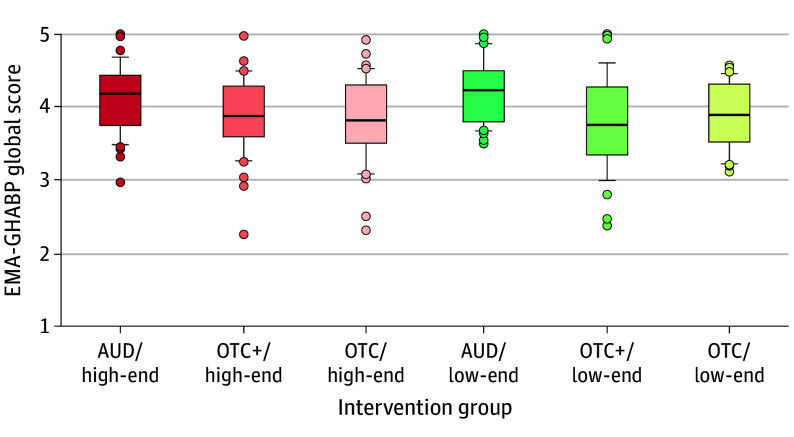
Main outcomes and measures: The primary outcome measure was the Glasgow Hearing Aid Benefit Profile (GHABP), which was administered using ecological momentary assessment (EMA). EMA-GHABP was conducted preintervention and throughout the seventh week postintervention.
Results: A total of 245 participants completed the study (121 women [49.4%]; mean [SD] age, 67.7 [8.1] years). After controlling for preintervention scores, the postintervention EMA-GHABP global score (ranging from 1 to 5) for AUD was significantly higher (indicating better outcomes) than for OTC+ and OTC by 0.33 points (95% CI, 0.14-0.52) and 0.32 points (95% CI, 0.13-0.51), respectively. The difference between OTC+ and OTC was not significant (0.02 points, 95% CI, -0.21 to 0.18). Nevertheless, EMA-GHABP global scores for OTC+ and OTC were close to 4 points, indicating positive outcomes. The effect of technology level and interaction between service model and technology level were not significant.
Conclusions and relevance: The trial results suggest that while OTC+ and OTC were effective, they did not achieve the same outcomes as AUD. As high-end and low-end HAs yielded similar outcomes, support for the higher cost of high-end HAs was not identified for individuals with mild to moderate hearing loss.
期刊介绍:
JAMA Otolaryngology–Head & Neck Surgery is a globally recognized and peer-reviewed medical journal dedicated to providing up-to-date information on diseases affecting the head and neck. It originated in 1925 as Archives of Otolaryngology and currently serves as the official publication for the American Head and Neck Society. As part of the prestigious JAMA Network, a collection of reputable general medical and specialty publications, it ensures the highest standards of research and expertise. Physicians and scientists worldwide rely on JAMA Otolaryngology–Head & Neck Surgery for invaluable insights in this specialized field.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


