Angiotensin-converting enzyme inhibitor-induced bowel angioedema: clinical features, diagnostic challenges, and recovery predictors from survival analysis: a systematic review of current reported cases.
{"title":"Angiotensin-converting enzyme inhibitor-induced bowel angioedema: clinical features, diagnostic challenges, and recovery predictors from survival analysis: a systematic review of current reported cases.","authors":"Thanathip Suenghataiphorn, Narisara Tribuddharat, Pojsakorn Danpanichkul, Narathorn Kulthamrongsri, Piyawat Kantagowit","doi":"10.20524/aog.2025.0967","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Angiotensin-converting enzyme inhibitor-induced bowel angioedema (ACEi-IAE) is a rare and frequently under-recognized condition. Its nonspecific gastrointestinal symptoms could lead to missed diagnoses, unnecessary procedures and inappropriate treatments. Given the scarcity of studies, we conducted a systematic review to summarize the clinical characteristics of ACEi-IAE, the diagnostic approach and factors predicting delayed recovery.</p><p><strong>Methods: </strong>Electronic databases, including MEDLINE, OVID and EMBASE, were used to identified eligible studies from inception to November 2024. Eligible cases were required to have a clear diagnosis of ACEi-IAE. Kaplan-Meier and multivariate Cox regression analyses were used to identify factors associated with delayed recovery time.</p><p><strong>Results: </strong>Our systematic review included 81 eligible studies, comprising 117 ACEi-IAE cases with a mean age of 50 years, of which 83% were female. Patients were mainly African Americans (50%) taking lisinopril (71%). All patients (100%) presented with abdominal pain and other non-specific features. The median recovery time was 48 h after discontinuing ACEi. Patients who had been taking lisinopril for a longer than average period (25.9 months) had a statistically significantly lower hazard ratio for recovery (adjusted hazard ratio [aHR] 0.39, 95% confidence interval [CI] 0.19-0.81; P=0.012), as did patients who had radiographic evidence of jejunal edema (aHR 0.29, 95%CI 0.11-0.74; P=0.010). Diagnostic criteria were proposed and summarized based on the findings.</p><p><strong>Conclusions: </strong>Clinicians should be aware of ACEi-induced bowel angioedema, particularly in ACEi users with non-specific abdominal pain. Implementation of our proposed diagnostic criteria is recommended to prevent unnecessary investigation and inappropriate treatment.</p>","PeriodicalId":7978,"journal":{"name":"Annals of Gastroenterology","volume":"38 3","pages":"276-283"},"PeriodicalIF":2.2000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12070344/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20524/aog.2025.0967","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/28 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Angiotensin-converting enzyme inhibitor-induced bowel angioedema (ACEi-IAE) is a rare and frequently under-recognized condition. Its nonspecific gastrointestinal symptoms could lead to missed diagnoses, unnecessary procedures and inappropriate treatments. Given the scarcity of studies, we conducted a systematic review to summarize the clinical characteristics of ACEi-IAE, the diagnostic approach and factors predicting delayed recovery.
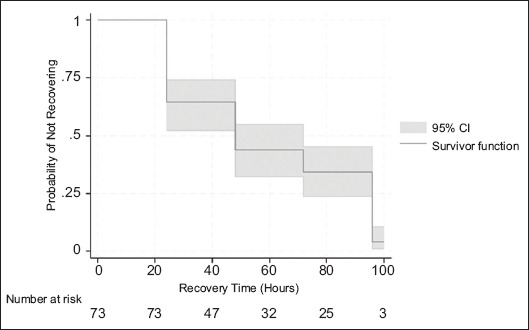
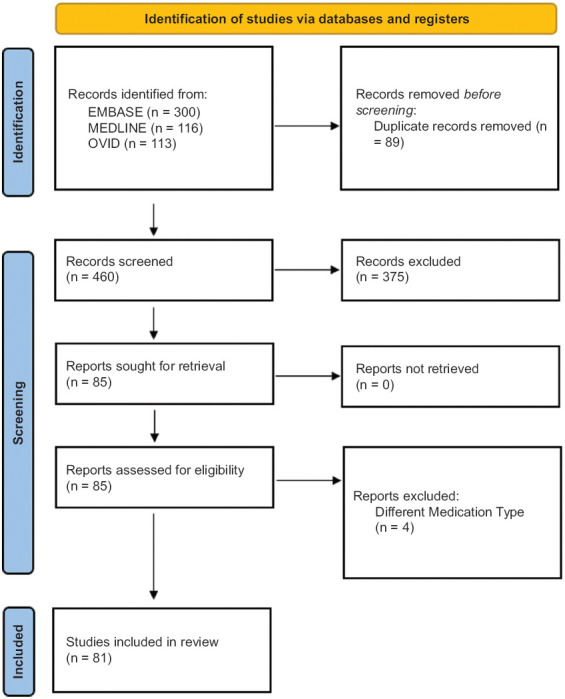
Methods: Electronic databases, including MEDLINE, OVID and EMBASE, were used to identified eligible studies from inception to November 2024. Eligible cases were required to have a clear diagnosis of ACEi-IAE. Kaplan-Meier and multivariate Cox regression analyses were used to identify factors associated with delayed recovery time.
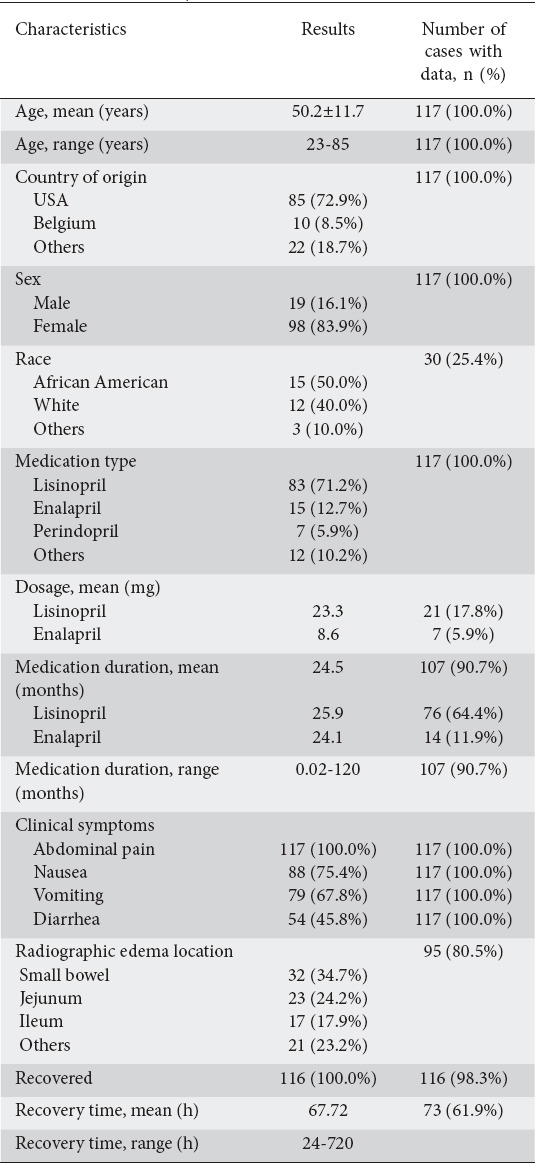
Results: Our systematic review included 81 eligible studies, comprising 117 ACEi-IAE cases with a mean age of 50 years, of which 83% were female. Patients were mainly African Americans (50%) taking lisinopril (71%). All patients (100%) presented with abdominal pain and other non-specific features. The median recovery time was 48 h after discontinuing ACEi. Patients who had been taking lisinopril for a longer than average period (25.9 months) had a statistically significantly lower hazard ratio for recovery (adjusted hazard ratio [aHR] 0.39, 95% confidence interval [CI] 0.19-0.81; P=0.012), as did patients who had radiographic evidence of jejunal edema (aHR 0.29, 95%CI 0.11-0.74; P=0.010). Diagnostic criteria were proposed and summarized based on the findings.
Conclusions: Clinicians should be aware of ACEi-induced bowel angioedema, particularly in ACEi users with non-specific abdominal pain. Implementation of our proposed diagnostic criteria is recommended to prevent unnecessary investigation and inappropriate treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


