{"title":"Biomarkers for successful tapering of a tumor necrosis factor inhibitor in patients with radiographic axial spondyloarthritis: A pilot study.","authors":"Hong Ki Min, Ji-Yeon Lee","doi":"10.1177/20503121251330812","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Tumor necrosis factor inhibitors are the most widely used biological disease-modifying antirheumatic drugs for radiographic axial spondyloarthritis. After achieving remission with tumor necrosis factor inhibitor treatment, experts recommend tapering tumor necrosis factor inhibitor. However, biomarkers for successful tumor necrosis factor inhibitor tapering in radiographic axial spondyloarthritis have not been identified.</p><p><strong>Objectives: </strong>To identify biomarkers associated with successful tumor necrosis factor inhibitor tapering in patients with radiographic axial spondyloarthritis.</p><p><strong>Design: </strong>We prospectively collected blood samples from radiographic axial spondyloarthritis patients at single tertiary hospital.</p><p><strong>Methods: </strong>Patients with radiographic axial spondyloarthritis who achieved remission (axial spondyloarthritis disease activity score < 1.3) after treatment with tumor necrosis factor inhibitor were enrolled. Baseline demographics, medication history, and laboratory data were collected when the tumor necrosis factor inhibitor dose was tapered. The percentage of helper T cell subtypes (Th1/Th2/Th17/Th22) in peripheral blood, and serum levels of tumor necrosis factor-α, interleukin-12, IL-17A, IL-22, IL-23, interferon (IFN)-γ, soluble CD14, and zonulin, were measured. Patients were assigned to tumor necrosis factor inhibitor tapering success (axial spondyloarthritis disease activity score < 2.1) or failure (axial spondyloarthritis disease activity score ⩾ 2.1) groups according to disease activity (assessed at 12 weeks posttumor necrosis factor inhibitor tapering).</p><p><strong>Results: </strong>Twenty radiographic axial spondyloarthritis patients were enrolled (median age, 31.0 years; 65% males). Most (80%) were positive for human leukocyte antigen-B27. The change of axial spondyloarthritis disease activity score in the tumor necrosis factor inhibitor-tapering failure group was 1.36, while that in the tumor necrosis factor inhibitor-tapering success group was 0.07. The percentage of Th1 and Th17 cells was significantly lower, and that of Th2 cells higher, in the tumor necrosis factor inhibitor-tapering success group. In addition, serum levels of IL-12, IL-17A, IL-22, IFN-γ, tumor necrosis factor-α, zonulin, and soluble CD14 were significantly lower in the tumor necrosis factor inhibitor-tapering success group.</p><p><strong>Conclusion: </strong>Patients with radiographic axial spondyloarthritis who achieve successful tumor necrosis factor inhibitor tapering had lower percentages of Th1 and Th17 cells, a higher percentage of Th2 cells, and lower serum levels of IL-12, IL-17A, IL-22, IFN-γ, tumor necrosis factor-α, zonulin, and soluble CD14 at the time of tumor necrosis factor inhibitor tapering. These findings may help to identify patients with radiographic axial spondyloarthritis for whom tumor necrosis factor inhibitor tapering is appropriate.</p>","PeriodicalId":21398,"journal":{"name":"SAGE Open Medicine","volume":"13 ","pages":"20503121251330812"},"PeriodicalIF":2.1000,"publicationDate":"2025-04-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12033542/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"SAGE Open Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20503121251330812","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Tumor necrosis factor inhibitors are the most widely used biological disease-modifying antirheumatic drugs for radiographic axial spondyloarthritis. After achieving remission with tumor necrosis factor inhibitor treatment, experts recommend tapering tumor necrosis factor inhibitor. However, biomarkers for successful tumor necrosis factor inhibitor tapering in radiographic axial spondyloarthritis have not been identified.
Objectives: To identify biomarkers associated with successful tumor necrosis factor inhibitor tapering in patients with radiographic axial spondyloarthritis.
Design: We prospectively collected blood samples from radiographic axial spondyloarthritis patients at single tertiary hospital.
Methods: Patients with radiographic axial spondyloarthritis who achieved remission (axial spondyloarthritis disease activity score < 1.3) after treatment with tumor necrosis factor inhibitor were enrolled. Baseline demographics, medication history, and laboratory data were collected when the tumor necrosis factor inhibitor dose was tapered. The percentage of helper T cell subtypes (Th1/Th2/Th17/Th22) in peripheral blood, and serum levels of tumor necrosis factor-α, interleukin-12, IL-17A, IL-22, IL-23, interferon (IFN)-γ, soluble CD14, and zonulin, were measured. Patients were assigned to tumor necrosis factor inhibitor tapering success (axial spondyloarthritis disease activity score < 2.1) or failure (axial spondyloarthritis disease activity score ⩾ 2.1) groups according to disease activity (assessed at 12 weeks posttumor necrosis factor inhibitor tapering).
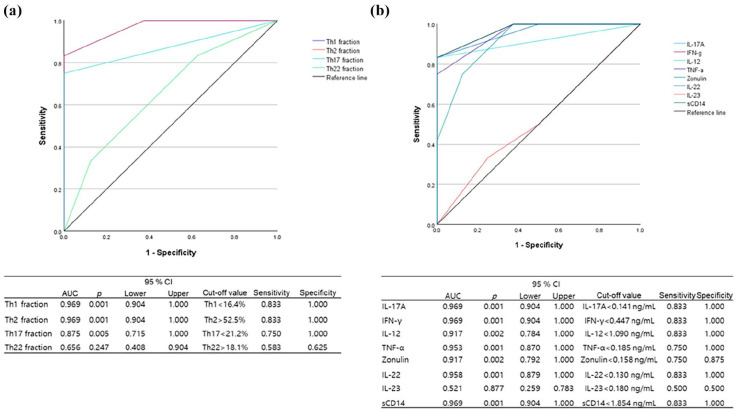
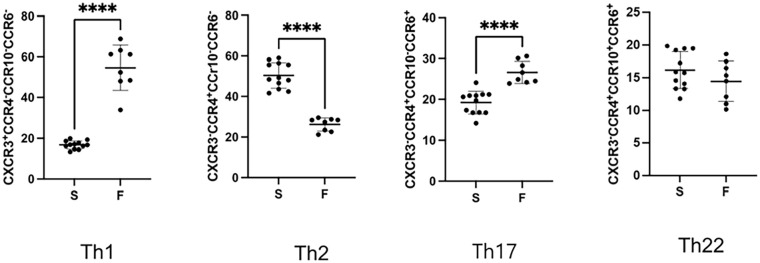
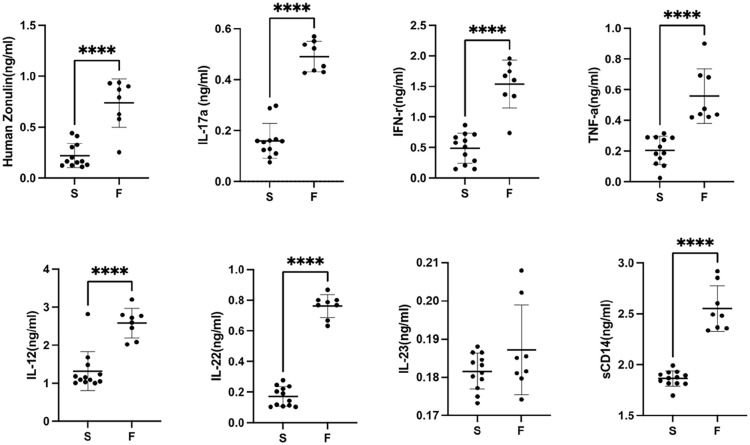
Results: Twenty radiographic axial spondyloarthritis patients were enrolled (median age, 31.0 years; 65% males). Most (80%) were positive for human leukocyte antigen-B27. The change of axial spondyloarthritis disease activity score in the tumor necrosis factor inhibitor-tapering failure group was 1.36, while that in the tumor necrosis factor inhibitor-tapering success group was 0.07. The percentage of Th1 and Th17 cells was significantly lower, and that of Th2 cells higher, in the tumor necrosis factor inhibitor-tapering success group. In addition, serum levels of IL-12, IL-17A, IL-22, IFN-γ, tumor necrosis factor-α, zonulin, and soluble CD14 were significantly lower in the tumor necrosis factor inhibitor-tapering success group.
Conclusion: Patients with radiographic axial spondyloarthritis who achieve successful tumor necrosis factor inhibitor tapering had lower percentages of Th1 and Th17 cells, a higher percentage of Th2 cells, and lower serum levels of IL-12, IL-17A, IL-22, IFN-γ, tumor necrosis factor-α, zonulin, and soluble CD14 at the time of tumor necrosis factor inhibitor tapering. These findings may help to identify patients with radiographic axial spondyloarthritis for whom tumor necrosis factor inhibitor tapering is appropriate.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


