Souleymane Diabate, Marco Arellano, Jonathan Cloutier, Michel Dallaire, Simon Plourde, Michel Labrecque
{"title":"Occlusive effectiveness of open-ended no-scalpel vasectomy with mucosal cautery and fascial interposition: a descriptive study.","authors":"Souleymane Diabate, Marco Arellano, Jonathan Cloutier, Michel Dallaire, Simon Plourde, Michel Labrecque","doi":"10.4103/aja202517","DOIUrl":null,"url":null,"abstract":"<p><strong>Abstract: </strong>We aimed to assess the occlusive effectiveness of open-ended vasectomy with mucosal cautery and fascial interposition and to determine the factors associated with occlusion failure. We studied all vasectomies performed between September 1, 2020, and August 31, 2021, by four vasectomy surgeons from Quebec City, Quebec, Canada. Sociodemographic and clinical characteristics were extracted from the electronic medical records. Occlusive effectiveness was assessed in all men with at least one postvasectomy semen analysis (PVSA). The effectiveness criteria were adapted from those of the American Urological Association (AUA) vasectomy guideline. Among the 4000 eligible vasectomies, 2242 (56.1%) were followed by at least one PVSA, with 99 (4.4%) requiring more than one PVSA. Occlusive effectiveness was achieved in 2233 vasectomies (99.6%; 95% confidence interval [CI]: 99.3%-99.8%), with 2199 (98.1%) and 34 (1.5%) classified as confirmed and probable success, respectively. The final status of the three vasectomies (0.1%) was indeterminate. Occlusive failure was observed in six vasectomies (0.3%; 95% CI: 0.1%-0.6%). The four surgeons had a similar risk of failure. The only significant factor associated with failure was the difficulty in performing the vas occlusion reported by the surgeon (7.4% [2/27] vs 0.2% [4/2212]; relative risk = 41.0; 95% CI: 7.8-214.2). The high occlusive effectiveness observed in our study validates AUA recommendations, supporting the use of this technique. Difficulty in occlusion of the vas deferens, as reported by surgeons, was the only factor associated with vasectomy failure. This finding highlights the need for PVSA in such cases.</p>","PeriodicalId":93889,"journal":{"name":"Asian journal of andrology","volume":" ","pages":"592-597"},"PeriodicalIF":2.7000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12422564/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Asian journal of andrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/aja202517","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/25 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
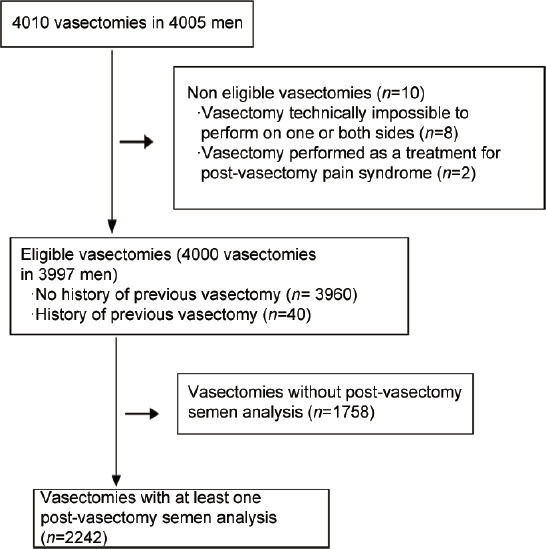
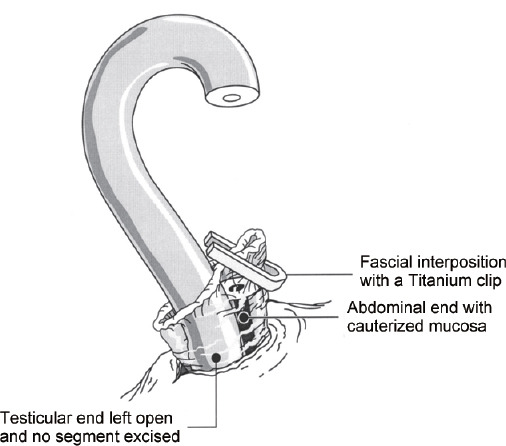
Abstract: We aimed to assess the occlusive effectiveness of open-ended vasectomy with mucosal cautery and fascial interposition and to determine the factors associated with occlusion failure. We studied all vasectomies performed between September 1, 2020, and August 31, 2021, by four vasectomy surgeons from Quebec City, Quebec, Canada. Sociodemographic and clinical characteristics were extracted from the electronic medical records. Occlusive effectiveness was assessed in all men with at least one postvasectomy semen analysis (PVSA). The effectiveness criteria were adapted from those of the American Urological Association (AUA) vasectomy guideline. Among the 4000 eligible vasectomies, 2242 (56.1%) were followed by at least one PVSA, with 99 (4.4%) requiring more than one PVSA. Occlusive effectiveness was achieved in 2233 vasectomies (99.6%; 95% confidence interval [CI]: 99.3%-99.8%), with 2199 (98.1%) and 34 (1.5%) classified as confirmed and probable success, respectively. The final status of the three vasectomies (0.1%) was indeterminate. Occlusive failure was observed in six vasectomies (0.3%; 95% CI: 0.1%-0.6%). The four surgeons had a similar risk of failure. The only significant factor associated with failure was the difficulty in performing the vas occlusion reported by the surgeon (7.4% [2/27] vs 0.2% [4/2212]; relative risk = 41.0; 95% CI: 7.8-214.2). The high occlusive effectiveness observed in our study validates AUA recommendations, supporting the use of this technique. Difficulty in occlusion of the vas deferens, as reported by surgeons, was the only factor associated with vasectomy failure. This finding highlights the need for PVSA in such cases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


