Anthony M Strada, Gus Suarez, Xian Luo-Owen, Maryam B Tabrizi, Martin G Rosenthal, Wesley T Stevens, Sharon S Lum, Kaushik Mukherjee
{"title":"Pragmatic O-Positive Whole-blood RandoMizaTion in male trauma Patients (POWeR-MTP).","authors":"Anthony M Strada, Gus Suarez, Xian Luo-Owen, Maryam B Tabrizi, Martin G Rosenthal, Wesley T Stevens, Sharon S Lum, Kaushik Mukherjee","doi":"10.1007/s00068-025-02848-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Hemorrhage is a significant cause of trauma-related death. Low-titer O-positive whole blood (LTOWB) is an alternative to component therapy (CT) [packed red blood cells (PRBC) and fresh frozen plasma (FFP)]. We evaluated if LTOWB reduces transfusion requirement or mortality.</p><p><strong>Methods: </strong>Adult male trauma activations requiring uncrossmatched transfusion in the emergency department underwent nonblinded 24-hour block randomization to receive uncrossmatched LTOWB or CT in the emergency department (ED). Female patients, children, and known prisoners were excluded. If LTOWB was not available, CT was used. Primary outcome was transfusion requirement in patients surviving ≥ 24 h, with a subset analysis for patients undergoing hemorrhage control interventions (HCI). Dichotomous variables were evaluated with Chi-Square testing and continuous outcomes with Student's T-test.</p><p><strong>Results: </strong>Overall, 199 patients were randomized (52 LTOWB, 147 CT); 36 patients (12 LTOWB, 24 CT) were excluded post-randomization for mortality within 24 h. The remaining 40 LTOWB and 123 CT patient cohorts had similar age, Glasgow Coma Scale, Injury Severity Score, heart rate, systolic blood pressure, and temperature. LTOWB patients received 1.4 ± 0.75 LTOWB units. LTOWB patients trended toward less transfusion (PRBC [3.8 ± 5.6 vs. 5.7 ± 6.2 units, p = 0.077], FFP [2.3 ± 3.8 vs. 3.5 ± 4.3 units, p = 0.088], and CRYO [0.13 ± 0.34 vs. 0.28 ± 0.68 units, p = 0.061]). Mortality was similar (LTOWB:10.2% [4/39] vs. CT:10.5% [13/123], p = 0.956). LTOWB patients undergoing HCI had less transfusion than CT patients (PRBC [3.9 ± 5.1 vs. 7.4 ± 7.2 units, p = 0.013]; in the HCI cohort the differences were even more pronounced when severe traumatic brain injury (TBI) deaths were excluded (PRBC [3.0 ± 3.6 vs. 7.4 ± 7.2 units, p < 0.001], FFP [2.1 ± 2.3 vs. 4.5 ± 5.2 units, p = 0.005]).</p><p><strong>Conclusion: </strong>LTOWB is associated with reduced PRBC transfusion in patients undergoing HCI, and a trend toward decreased PRBC, FFP, and CRYO transfusion in all patients.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov (NCT05081063), posted 10/18/2021.</p>","PeriodicalId":12064,"journal":{"name":"European Journal of Trauma and Emergency Surgery","volume":"51 1","pages":"175"},"PeriodicalIF":2.2000,"publicationDate":"2025-04-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12003594/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Trauma and Emergency Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00068-025-02848-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Hemorrhage is a significant cause of trauma-related death. Low-titer O-positive whole blood (LTOWB) is an alternative to component therapy (CT) [packed red blood cells (PRBC) and fresh frozen plasma (FFP)]. We evaluated if LTOWB reduces transfusion requirement or mortality.
Methods: Adult male trauma activations requiring uncrossmatched transfusion in the emergency department underwent nonblinded 24-hour block randomization to receive uncrossmatched LTOWB or CT in the emergency department (ED). Female patients, children, and known prisoners were excluded. If LTOWB was not available, CT was used. Primary outcome was transfusion requirement in patients surviving ≥ 24 h, with a subset analysis for patients undergoing hemorrhage control interventions (HCI). Dichotomous variables were evaluated with Chi-Square testing and continuous outcomes with Student's T-test.
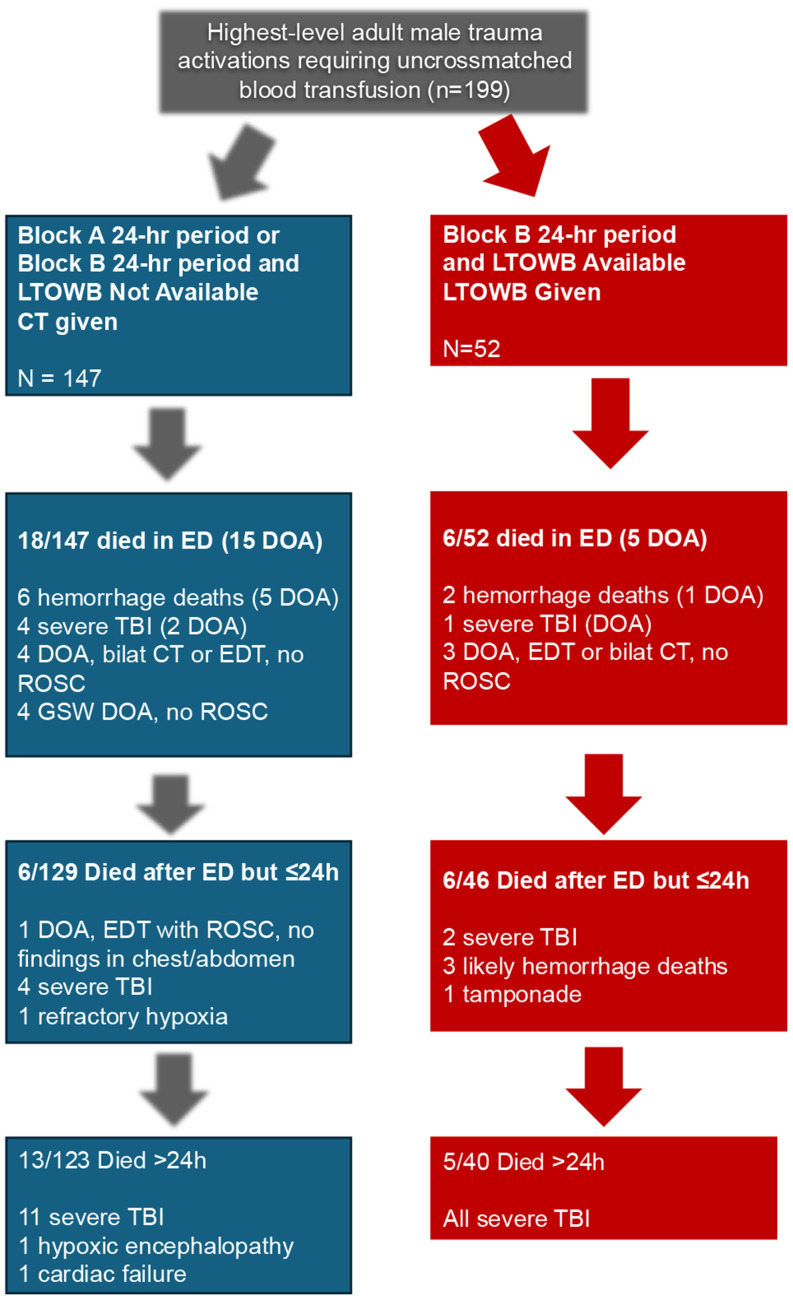
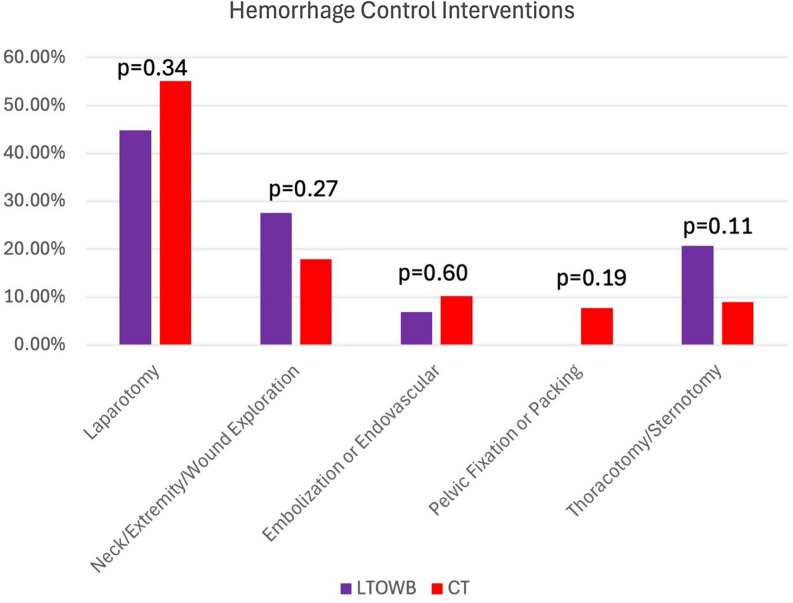
Results: Overall, 199 patients were randomized (52 LTOWB, 147 CT); 36 patients (12 LTOWB, 24 CT) were excluded post-randomization for mortality within 24 h. The remaining 40 LTOWB and 123 CT patient cohorts had similar age, Glasgow Coma Scale, Injury Severity Score, heart rate, systolic blood pressure, and temperature. LTOWB patients received 1.4 ± 0.75 LTOWB units. LTOWB patients trended toward less transfusion (PRBC [3.8 ± 5.6 vs. 5.7 ± 6.2 units, p = 0.077], FFP [2.3 ± 3.8 vs. 3.5 ± 4.3 units, p = 0.088], and CRYO [0.13 ± 0.34 vs. 0.28 ± 0.68 units, p = 0.061]). Mortality was similar (LTOWB:10.2% [4/39] vs. CT:10.5% [13/123], p = 0.956). LTOWB patients undergoing HCI had less transfusion than CT patients (PRBC [3.9 ± 5.1 vs. 7.4 ± 7.2 units, p = 0.013]; in the HCI cohort the differences were even more pronounced when severe traumatic brain injury (TBI) deaths were excluded (PRBC [3.0 ± 3.6 vs. 7.4 ± 7.2 units, p < 0.001], FFP [2.1 ± 2.3 vs. 4.5 ± 5.2 units, p = 0.005]).
Conclusion: LTOWB is associated with reduced PRBC transfusion in patients undergoing HCI, and a trend toward decreased PRBC, FFP, and CRYO transfusion in all patients.
期刊介绍:
The European Journal of Trauma and Emergency Surgery aims to open an interdisciplinary forum that allows for the scientific exchange between basic and clinical science related to pathophysiology, diagnostics and treatment of traumatized patients. The journal covers all aspects of clinical management, operative treatment and related research of traumatic injuries.
Clinical and experimental papers on issues relevant for the improvement of trauma care are published. Reviews, original articles, short communications and letters allow the appropriate presentation of major and minor topics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


