Lamia Alakrash, Lama Alzamil, Mohammed Aljughayman, Salman Almalki
{"title":"Pityriasis rosea-like eruption induced by omalizumab: a case report of a rare side effect.","authors":"Lamia Alakrash, Lama Alzamil, Mohammed Aljughayman, Salman Almalki","doi":"10.21037/acr-24-114","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Omalizumab is a monoclonal humanized antibody used as a third-line treatment for chronic spontaneous urticaria (CSU). While it has shown significant efficacy in controlling urticaria symptoms, it is also associated with various adverse effects. Cutaneous side effects of omalizumab have been reported, but the mechanisms underlying these reactions are not fully understood. This case report describes a patient who developed a maculopapular rash after receiving the 8th dose of omalizumab, which has not been previously reported.</p><p><strong>Case description: </strong>The patient in this case was a 46-year-old male with CSU who had been receiving omalizumab injections every four weeks. After the 8th dose, he developed a generalized itchy erythematous skin eruption six days after the injection. The rash progressively worsened over a two-week period. Interestingly, the patient had experienced a milder skin reaction after the 6th dose, which resolved on its own. A skin biopsy showed mild interstitial edema in the dermis with a mild perivascular infiltrate of lymphocytes and eosinophils, consistent with a drug-induced eruption. The patient was advised to hold the next dose of omalizumab and was managed with topical steroids. Significant improvement and resolution of the lesions were observed, and no recurrence or relapse was reported after the patient resumed omalizumab.</p><p><strong>Conclusions: </strong>This case adds to the existing literature by reporting a pityriasis rosea-like eruption as an adverse reaction to omalizumab, which has not been extensively documented. The delayed onset and progressive nature of the rash after the 8th dose, as well as the milder previous reaction after the 6th dose, highlight the importance of considering omalizumab as a potential cause of various cutaneous reactions. Physicians should be vigilant in monitoring patients receiving omalizumab for any signs of skin eruptions or other adverse effects. Further research is needed to understand the mechanisms underlying cutaneous reactions to omalizumab and to establish guidelines for their management. This case emphasizes the need for ongoing attention to potential side effects or reactions in patients receiving omalizumab.</p>","PeriodicalId":29752,"journal":{"name":"AME Case Reports","volume":"9 ","pages":"65"},"PeriodicalIF":0.7000,"publicationDate":"2025-04-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12053656/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AME Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/acr-24-114","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Omalizumab is a monoclonal humanized antibody used as a third-line treatment for chronic spontaneous urticaria (CSU). While it has shown significant efficacy in controlling urticaria symptoms, it is also associated with various adverse effects. Cutaneous side effects of omalizumab have been reported, but the mechanisms underlying these reactions are not fully understood. This case report describes a patient who developed a maculopapular rash after receiving the 8th dose of omalizumab, which has not been previously reported.
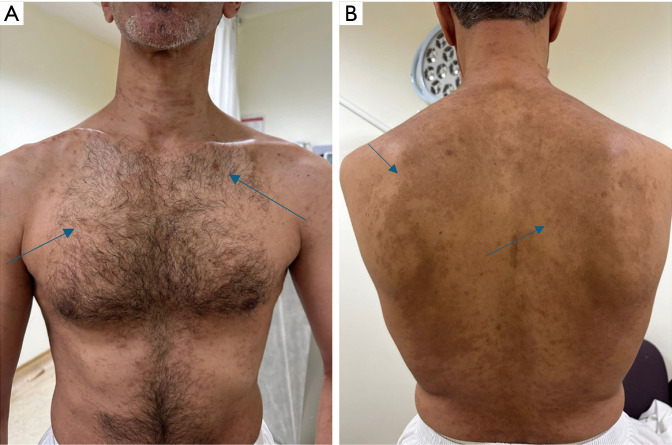
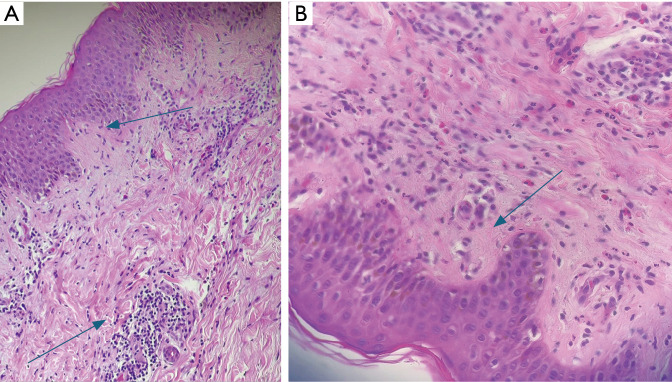
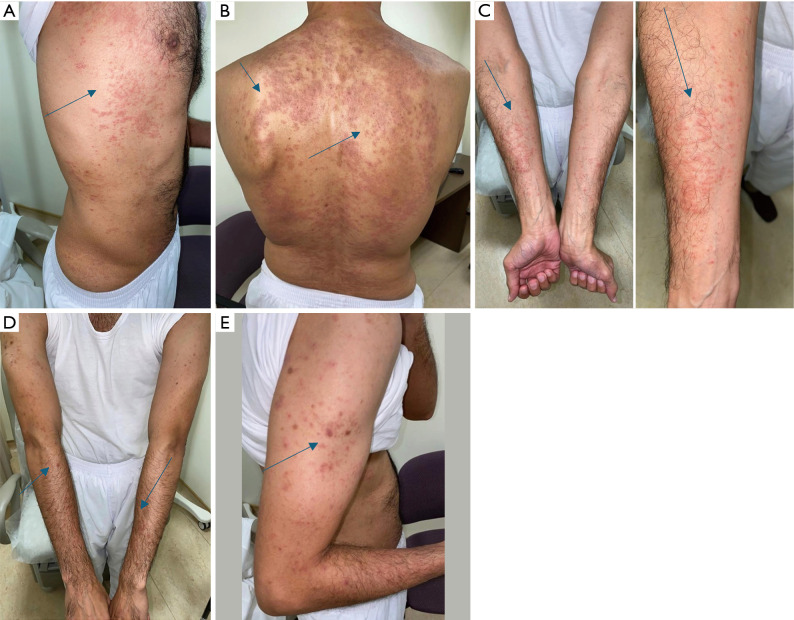
Case description: The patient in this case was a 46-year-old male with CSU who had been receiving omalizumab injections every four weeks. After the 8th dose, he developed a generalized itchy erythematous skin eruption six days after the injection. The rash progressively worsened over a two-week period. Interestingly, the patient had experienced a milder skin reaction after the 6th dose, which resolved on its own. A skin biopsy showed mild interstitial edema in the dermis with a mild perivascular infiltrate of lymphocytes and eosinophils, consistent with a drug-induced eruption. The patient was advised to hold the next dose of omalizumab and was managed with topical steroids. Significant improvement and resolution of the lesions were observed, and no recurrence or relapse was reported after the patient resumed omalizumab.
Conclusions: This case adds to the existing literature by reporting a pityriasis rosea-like eruption as an adverse reaction to omalizumab, which has not been extensively documented. The delayed onset and progressive nature of the rash after the 8th dose, as well as the milder previous reaction after the 6th dose, highlight the importance of considering omalizumab as a potential cause of various cutaneous reactions. Physicians should be vigilant in monitoring patients receiving omalizumab for any signs of skin eruptions or other adverse effects. Further research is needed to understand the mechanisms underlying cutaneous reactions to omalizumab and to establish guidelines for their management. This case emphasizes the need for ongoing attention to potential side effects or reactions in patients receiving omalizumab.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


