{"title":"General Anesthesia Surgery for Early Breast Cancer in a Patient with Severe Heart Failure due to Dilated Cardiomyopathy: A Case Report.","authors":"Tomohiro Oshino, Karin Shikishima, Yumi Moriya, Mitsuchika Hosoda, Kiwamu Kamiya, Toshiyuki Nagai, Toshihisa Anzai, Masato Takahashi","doi":"10.70352/scrj.cr.25-0034","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Perioperative mortality is significantly higher in cases of heart failure with severe left ventricular ejection fraction (LVEF) reduction, making it challenging to decide whether to proceed with surgery for early-stage breast cancer, which is not immediately fatal. However, the prognosis of heart failure has improved and breast cancer is increasingly becoming a prognostic factor. Herein, we report the case of a breast cancer patient with severe heart failure due to dilated cardiomyopathy (DC), who was deemed fit to undergo surgery under general anesthesia after obtaining sufficient informed consent and achieving improvement in heart failure symptoms during endocrine therapy.</p><p><strong>Case presentation: </strong>A 64-year-old female with a history of DC and sustained ventricular tachycardia, who had received cardiac resynchronization therapy with defibrillator implantation, underwent breast cancer surgery. She had been repeatedly hospitalized for heart failure with an LVEF of 19% and New York Heart Association (NYHA) Class III status, and heart transplant surgery was considered. However, a screening computed tomography scan revealed right breast cancer, and neither heart transplantation nor breast cancer surgery was performed. Endocrine therapy was initiated and failed 48 months after administration. Although the LVEF remained low at 21%, the NYHA classification improved to Class II, and she had not been hospitalized for heart failure for an extended period since her breast cancer diagnosis. Therefore, breast cancer surgery was performed under general anesthesia and no postoperative complications were observed throughout the course of the surgery.</p><p><strong>Conclusion: </strong>Given that the prognosis for heart failure may statistically be better than that for breast cancer, early breast cancer surgery should be performed in patients with stable heart failure symptoms.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"11 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12006746/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.70352/scrj.cr.25-0034","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/9 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Perioperative mortality is significantly higher in cases of heart failure with severe left ventricular ejection fraction (LVEF) reduction, making it challenging to decide whether to proceed with surgery for early-stage breast cancer, which is not immediately fatal. However, the prognosis of heart failure has improved and breast cancer is increasingly becoming a prognostic factor. Herein, we report the case of a breast cancer patient with severe heart failure due to dilated cardiomyopathy (DC), who was deemed fit to undergo surgery under general anesthesia after obtaining sufficient informed consent and achieving improvement in heart failure symptoms during endocrine therapy.
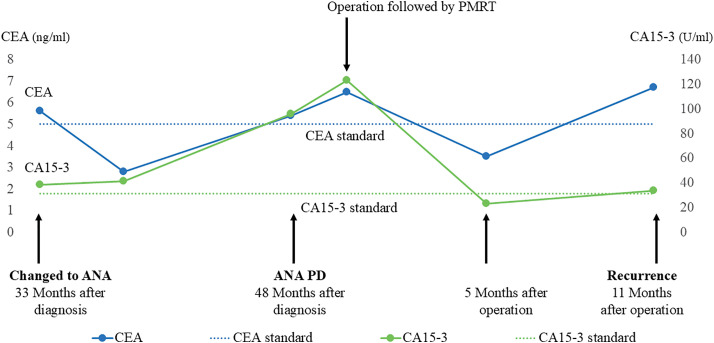
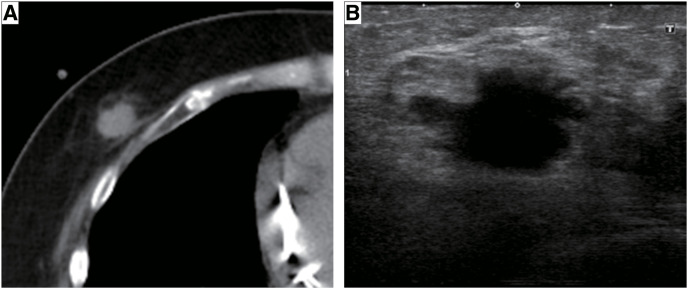
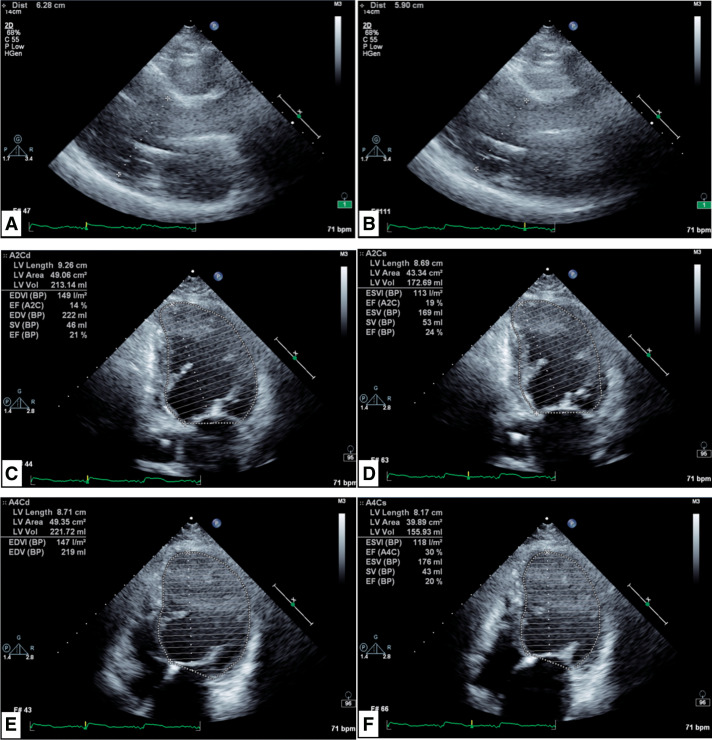
Case presentation: A 64-year-old female with a history of DC and sustained ventricular tachycardia, who had received cardiac resynchronization therapy with defibrillator implantation, underwent breast cancer surgery. She had been repeatedly hospitalized for heart failure with an LVEF of 19% and New York Heart Association (NYHA) Class III status, and heart transplant surgery was considered. However, a screening computed tomography scan revealed right breast cancer, and neither heart transplantation nor breast cancer surgery was performed. Endocrine therapy was initiated and failed 48 months after administration. Although the LVEF remained low at 21%, the NYHA classification improved to Class II, and she had not been hospitalized for heart failure for an extended period since her breast cancer diagnosis. Therefore, breast cancer surgery was performed under general anesthesia and no postoperative complications were observed throughout the course of the surgery.
Conclusion: Given that the prognosis for heart failure may statistically be better than that for breast cancer, early breast cancer surgery should be performed in patients with stable heart failure symptoms.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


