Associations Between Mean Arterial Pressure and Prognosis in Acute Myocardial Infarction Complicated by Cardiogenic Shock Differ Depending on Coma Status.
{"title":"Associations Between Mean Arterial Pressure and Prognosis in Acute Myocardial Infarction Complicated by Cardiogenic Shock Differ Depending on Coma Status.","authors":"Keishi Moriwaki, Tairo Kurita, Kazuma Yamaguchi, Kenta Uno, Yumi Hirota, Masashi Yanagisawa, Ryo Okado, Hiromasa Ito, Takashi Kato, Shusuke Fukuoka, Akihiro Takasaki, Kentaro Kakuta, Naoki Fujimoto, Takashi Yamanaka, Ryuji Okamoto, Kaoru Dohi","doi":"10.1253/circrep.CR-25-0001","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In acute myocardial infarction complicated by cardiogenic shock (AMI-CS), low mean arterial pressure (MAP) can reduce cerebral perfusion, potentially resulting in coma. While both MAP and coma on admission are critical prognostic factors, the relationship between them and their prognostic significance based on coma status remains unclear.</p><p><strong>Methods and results: </strong>A retrospective analysis of 543 AMI-CS patients was conducted. The overall median MAP was 77 mmHg, with no significant difference between the coma and non-coma groups. The coma group had a higher 30-day mortality compared with the non-coma group (50% vs. 29%; P<0.001). The area under the curve for MAP predicting 30-day mortality was 0.723 (P<0.001) in the coma group, with a cut-off MAP of 76.3 mmHg (sensitivity 0.66, specificity 0.69), but was insignificant in the non-coma group (AUC 0.543; P=0.176). Kaplan-Meier analysis showed higher mortality with low MAP (<77 mmHg) in the coma group, whereas MAP had no significant impact in the non-coma group. Multivariate Cox regression identified low MAP as an independent prognostic factor in the coma group only.</p><p><strong>Conclusions: </strong>The associations between MAP and prognosis differ depending on the coma status in AMI-CS. Low MAP is a prognostic factor for mortality only in patients with coma. This study highlights the need for treatment strategies tailored to neurological status.</p>","PeriodicalId":94305,"journal":{"name":"Circulation reports","volume":"7 4","pages":"247-256"},"PeriodicalIF":1.1000,"publicationDate":"2025-03-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11981676/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1253/circrep.CR-25-0001","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/10 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In acute myocardial infarction complicated by cardiogenic shock (AMI-CS), low mean arterial pressure (MAP) can reduce cerebral perfusion, potentially resulting in coma. While both MAP and coma on admission are critical prognostic factors, the relationship between them and their prognostic significance based on coma status remains unclear.
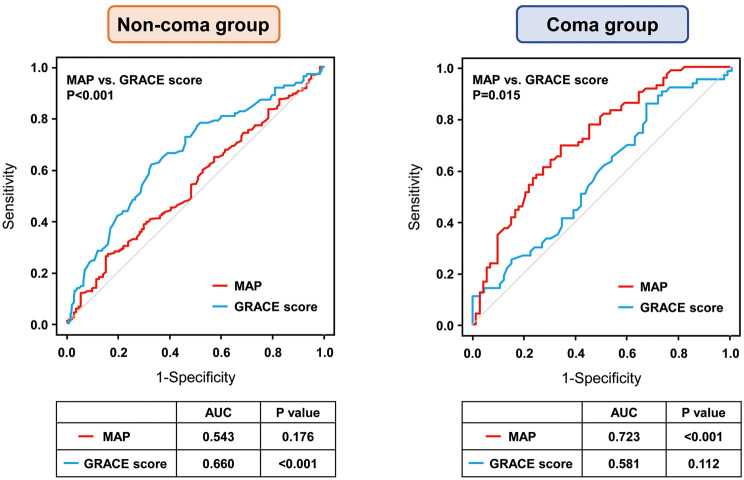
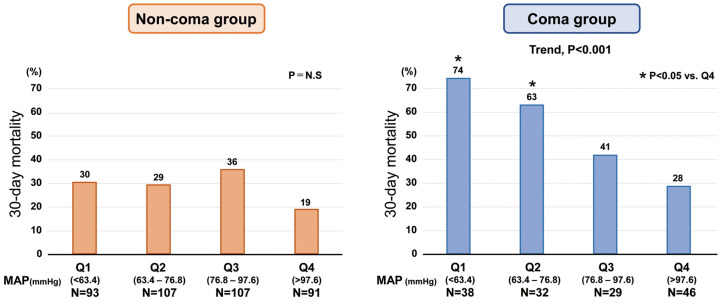
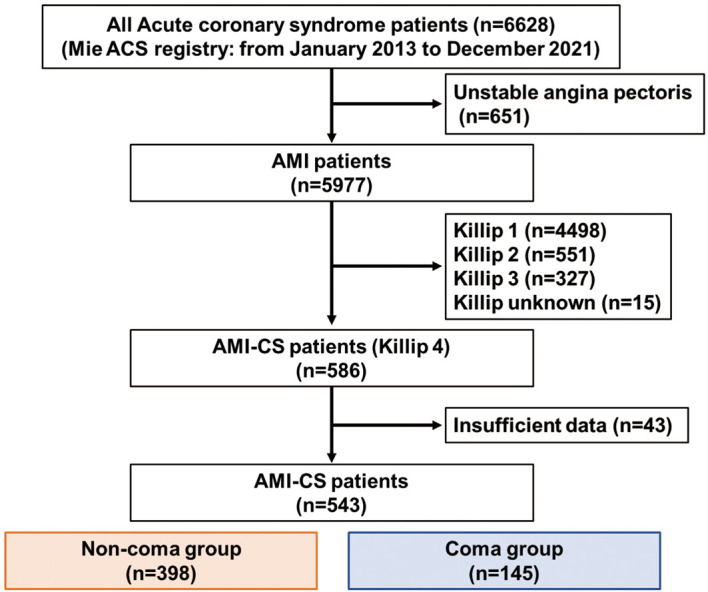
Methods and results: A retrospective analysis of 543 AMI-CS patients was conducted. The overall median MAP was 77 mmHg, with no significant difference between the coma and non-coma groups. The coma group had a higher 30-day mortality compared with the non-coma group (50% vs. 29%; P<0.001). The area under the curve for MAP predicting 30-day mortality was 0.723 (P<0.001) in the coma group, with a cut-off MAP of 76.3 mmHg (sensitivity 0.66, specificity 0.69), but was insignificant in the non-coma group (AUC 0.543; P=0.176). Kaplan-Meier analysis showed higher mortality with low MAP (<77 mmHg) in the coma group, whereas MAP had no significant impact in the non-coma group. Multivariate Cox regression identified low MAP as an independent prognostic factor in the coma group only.
Conclusions: The associations between MAP and prognosis differ depending on the coma status in AMI-CS. Low MAP is a prognostic factor for mortality only in patients with coma. This study highlights the need for treatment strategies tailored to neurological status.
背景:急性心肌梗死合并心源性休克(AMI-CS)时,低平均动脉压(MAP)可减少脑灌注,可能导致昏迷。虽然MAP和入院时昏迷都是关键的预后因素,但它们之间的关系及其基于昏迷状态的预后意义尚不清楚。方法与结果:对543例AMI-CS患者进行回顾性分析。总体中位MAP为77 mmHg,昏迷组和非昏迷组之间无显著差异。昏迷组的30天死亡率高于非昏迷组(50% vs 29%;结论:AMI-CS患者的昏迷状态不同,MAP与预后的关系也不同。低MAP仅是昏迷患者死亡的预后因素。这项研究强调了针对神经系统状况量身定制治疗策略的必要性。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


