Vanita R Aroda, Nils B Jørgensen, Bharath Kumar, Ildiko Lingvay, Anne Sofie Laulund, John B Buse
{"title":"High-Dose Semaglutide (Up to 16 mg) in People With Type 2 Diabetes and Overweight or Obesity: A Randomized, Placebo-Controlled, Phase 2 Trial.","authors":"Vanita R Aroda, Nils B Jørgensen, Bharath Kumar, Ildiko Lingvay, Anne Sofie Laulund, John B Buse","doi":"10.2337/dc24-2425","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Studies have demonstrated dose-dependent efficacy of glucagon-like peptide 1 receptor agonists for glycemic control and body weight. The aim of this trial was to characterize the dose-dependent effects of semaglutide (up to 16 mg/week) in people with type 2 diabetes and overweight or obesity.</p><p><strong>Research design and methods: </strong>In this parallel-group, participant- and investigator-blinded, phase 2 trial, 245 individuals with type 2 diabetes and BMI ≥27 kg/m2 on metformin were randomized to weekly semaglutide (2, 8, or 16 mg s.c.) or placebo for 40 weeks. Doses were escalated every 4 weeks, followed by a maintenance period. Dose modifications were not allowed. Primary and secondary efficacy end points included change from baseline to week 40 in HbA1c and body weight, respectively.</p><p><strong>Results: </strong>Estimated treatment difference between 16 and 2 mg was -0.3 percentage points (%-points) (95% CI -0.7 to 0.2; P = 0.245) for HbA1c change and -3.4 kg (-6.0 to -0.8; P = 0.011) for weight change for the treatment policy estimand and -0.5%-points (-1.0 to -0.1; P = 0.015) and -4.5 kg (-7.6 to -1.4; P = 0.004), respectively, for the hypothetical estimand. Dose-response modeling confirmed these findings. Treatment-emergent adverse events (AEs) and treatment discontinuations due to AEs, primarily gastrointestinal, were more frequent in the semaglutide 8 and 16 mg groups than in the 2 mg group. No severe hypoglycemic episodes were reported.</p><p><strong>Conclusions: </strong>Higher semaglutide doses for type 2 diabetes and overweight or obesity provide modest additional glucose-lowering effect, with additional weight loss, at the expense of more AEs and treatment discontinuations. A study for evaluating high-dose semaglutide in obesity is currently underway.</p>","PeriodicalId":93979,"journal":{"name":"Diabetes care","volume":" ","pages":"905-913"},"PeriodicalIF":16.6000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12094194/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diabetes care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2337/dc24-2425","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Studies have demonstrated dose-dependent efficacy of glucagon-like peptide 1 receptor agonists for glycemic control and body weight. The aim of this trial was to characterize the dose-dependent effects of semaglutide (up to 16 mg/week) in people with type 2 diabetes and overweight or obesity.
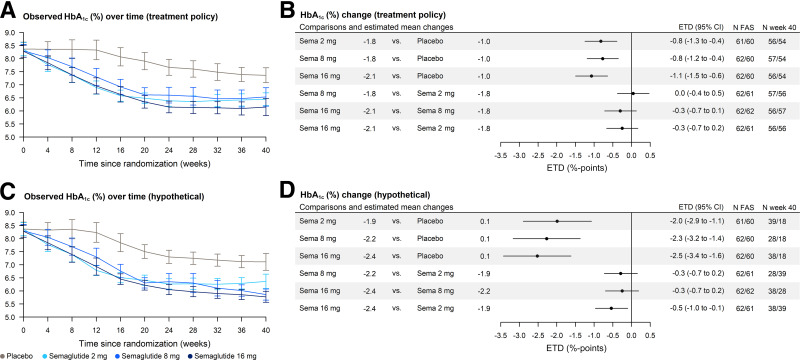
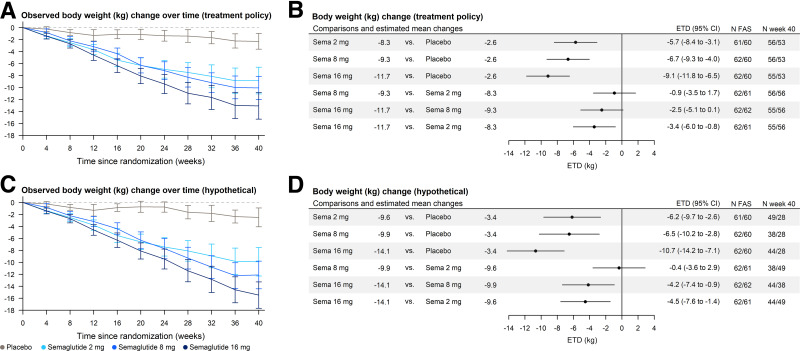
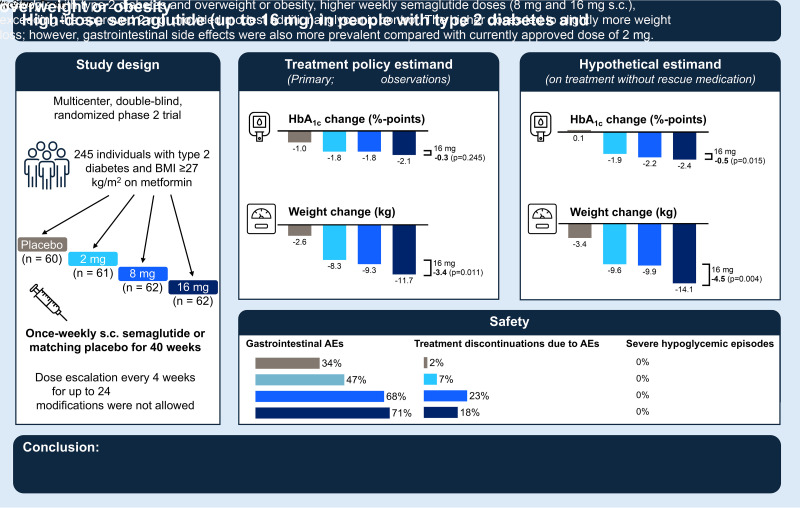
Research design and methods: In this parallel-group, participant- and investigator-blinded, phase 2 trial, 245 individuals with type 2 diabetes and BMI ≥27 kg/m2 on metformin were randomized to weekly semaglutide (2, 8, or 16 mg s.c.) or placebo for 40 weeks. Doses were escalated every 4 weeks, followed by a maintenance period. Dose modifications were not allowed. Primary and secondary efficacy end points included change from baseline to week 40 in HbA1c and body weight, respectively.
Results: Estimated treatment difference between 16 and 2 mg was -0.3 percentage points (%-points) (95% CI -0.7 to 0.2; P = 0.245) for HbA1c change and -3.4 kg (-6.0 to -0.8; P = 0.011) for weight change for the treatment policy estimand and -0.5%-points (-1.0 to -0.1; P = 0.015) and -4.5 kg (-7.6 to -1.4; P = 0.004), respectively, for the hypothetical estimand. Dose-response modeling confirmed these findings. Treatment-emergent adverse events (AEs) and treatment discontinuations due to AEs, primarily gastrointestinal, were more frequent in the semaglutide 8 and 16 mg groups than in the 2 mg group. No severe hypoglycemic episodes were reported.
Conclusions: Higher semaglutide doses for type 2 diabetes and overweight or obesity provide modest additional glucose-lowering effect, with additional weight loss, at the expense of more AEs and treatment discontinuations. A study for evaluating high-dose semaglutide in obesity is currently underway.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


