Peerapon Kiatkittikul, Teemu Maaniitty, Sarah Bär, Takeru Nabeta, Jeroen J Bax, Antti Saraste, Juhani Knuuti
{"title":"Factors affecting the performance of a novel artificial intelligence-based coronary computed tomography-derived ischaemia algorithm.","authors":"Peerapon Kiatkittikul, Teemu Maaniitty, Sarah Bär, Takeru Nabeta, Jeroen J Bax, Antti Saraste, Juhani Knuuti","doi":"10.1093/ehjimp/qyaf033","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>AI-QCT<sub>ischaemia</sub> is an FDA-cleared novel artificial intelligence-guided method that utilizes features from coronary computed tomography angiography (CCTA) to predict myocardial ischaemia.</p><p><strong>Objective: </strong>To identify factors associated with discrepancy between AI-QCT<sub>ischaemia</sub> and positron emission tomography (PET) perfusion.</p><p><strong>Methods and results: </strong>Six hundred and sixty-two patients with suspected obstructive coronary artery disease (CAD) on CCTA and undergoing [<sup>15</sup>O]H<sub>2</sub>O PET were analysed using AI-QCT<sub>ischaemia</sub>. Multivariable logistic regression identified factors associated with discrepancy. Perfusion homogeneity was measured by relative flow reserve. A total of 209 (32%) patients showed discrepancies: 62 (9%) exhibited normal AI-QCT<sub>ischaemia</sub> but abnormal perfusion (false negative AI-QCT<sub>ischaemia</sub>), whereas 147 (22%) had abnormal AI-QCT<sub>ischaemia</sub> despite normal perfusion (false positive AI-QCT<sub>ischaemia</sub>). False positive AI-QCT<sub>ischaemia</sub> patients (vs. true positive) were more often females, older, with less typical angina, and less advanced CAD. In multivariable analysis, typical angina [OR 95% CI: 1.796 (1.015-3.179), <i>P</i> = 0.044], diameter stenosis per 1% increase [1.058 (1.036-1.080), <i>P</i> < 0.001], and percent atheroma volume per 1% increase [1.103 (1.051-1.158), <i>P</i> < 0.001] significantly predicted true positive, while age was inversely associated [0.955 (0.923-0.989), <i>P</i> = 0.010]. False-negative AI-QCT<sub>ischaemia</sub> patients (vs. true negative) were more often males, smokers, with less good CCTA image quality, and more advanced CAD. However, none was significant in multivariable analysis. Furthermore, false-negative AI-QCT<sub>ischaemia</sub> showed more homogenously reduced perfusion by relative flow reserve compared to true positive (median ± IQR: 0.68 ± 0.15 vs. 0.56 ± 0.23, <i>P</i> < 0.001) and 21 (34%) of false negative showed globally reduced perfusion.</p><p><strong>Conclusion: </strong>For abnormal AI-QCT<sub>ischaemia</sub>, younger age, typical angina, more severe stenosis, and more extensive atherosclerosis predicted abnormal PET perfusion. With false negative AI-QCT<sub>ischaemia</sub>, perfusion abnormalities were partly explained by microvascular disease.</p>","PeriodicalId":94317,"journal":{"name":"European heart journal. Imaging methods and practice","volume":"2 4","pages":"qyaf033"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12003262/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Imaging methods and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjimp/qyaf033","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: AI-QCTischaemia is an FDA-cleared novel artificial intelligence-guided method that utilizes features from coronary computed tomography angiography (CCTA) to predict myocardial ischaemia.
Objective: To identify factors associated with discrepancy between AI-QCTischaemia and positron emission tomography (PET) perfusion.
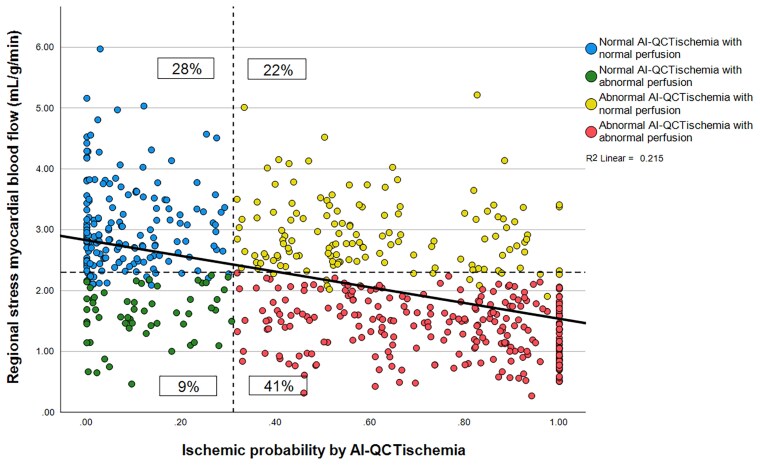
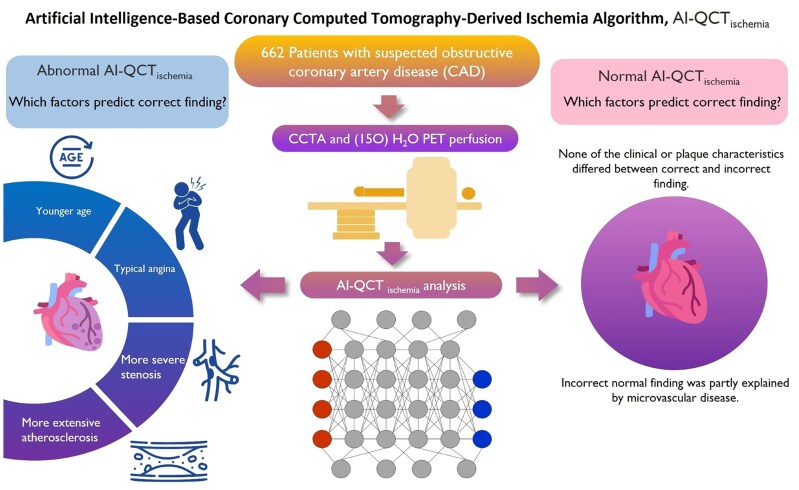
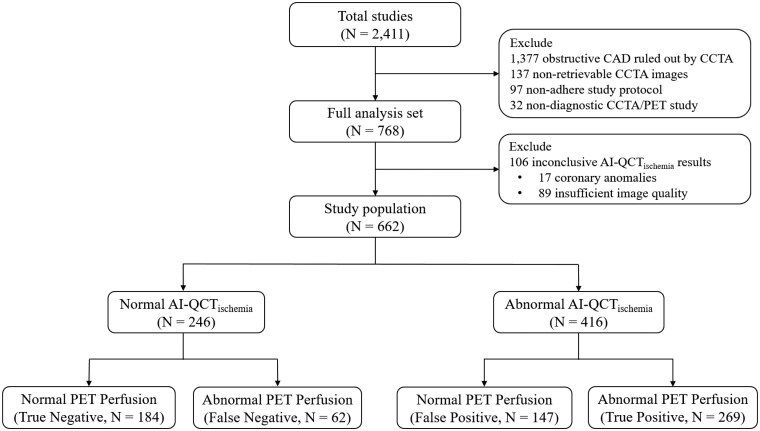
Methods and results: Six hundred and sixty-two patients with suspected obstructive coronary artery disease (CAD) on CCTA and undergoing [15O]H2O PET were analysed using AI-QCTischaemia. Multivariable logistic regression identified factors associated with discrepancy. Perfusion homogeneity was measured by relative flow reserve. A total of 209 (32%) patients showed discrepancies: 62 (9%) exhibited normal AI-QCTischaemia but abnormal perfusion (false negative AI-QCTischaemia), whereas 147 (22%) had abnormal AI-QCTischaemia despite normal perfusion (false positive AI-QCTischaemia). False positive AI-QCTischaemia patients (vs. true positive) were more often females, older, with less typical angina, and less advanced CAD. In multivariable analysis, typical angina [OR 95% CI: 1.796 (1.015-3.179), P = 0.044], diameter stenosis per 1% increase [1.058 (1.036-1.080), P < 0.001], and percent atheroma volume per 1% increase [1.103 (1.051-1.158), P < 0.001] significantly predicted true positive, while age was inversely associated [0.955 (0.923-0.989), P = 0.010]. False-negative AI-QCTischaemia patients (vs. true negative) were more often males, smokers, with less good CCTA image quality, and more advanced CAD. However, none was significant in multivariable analysis. Furthermore, false-negative AI-QCTischaemia showed more homogenously reduced perfusion by relative flow reserve compared to true positive (median ± IQR: 0.68 ± 0.15 vs. 0.56 ± 0.23, P < 0.001) and 21 (34%) of false negative showed globally reduced perfusion.
Conclusion: For abnormal AI-QCTischaemia, younger age, typical angina, more severe stenosis, and more extensive atherosclerosis predicted abnormal PET perfusion. With false negative AI-QCTischaemia, perfusion abnormalities were partly explained by microvascular disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


