Effect of Antibiotics With Anaerobic Coverage on Graft-Versus-Host Disease in Patients Undergoing Allogeneic Hematopoietic Stem Cell Transplantation: A Systematic Review and Meta-Analysis.
{"title":"Effect of Antibiotics With Anaerobic Coverage on Graft-Versus-Host Disease in Patients Undergoing Allogeneic Hematopoietic Stem Cell Transplantation: A Systematic Review and Meta-Analysis.","authors":"Hiroshi Ito, Yui Okamura, Yuna Tomura, Jura Oshida, Minori Fujita, Daiki Kobayashi","doi":"10.1111/tid.70049","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Broad-spectrum antibiotics are standard for febrile neutropenia (FN) in allogeneic hematopoietic stem cell transplantation (HSCT) but may disrupt gut microbiota, increasing the risk of graft-versus-host disease (GVHD). However, current evidence on the effects of anaerobic versus limited anaerobic antibiotic coverage on GVHD-related outcomes remains inconclusive.</p><p><strong>Methods: </strong>We systematically searched for studies assessing overall survival, acute GVHD incidence, and GVHD-related mortality in patients with allogeneic HSCT receiving antibiotics with anaerobic versus limited anaerobic coverage. A random-effects meta-analysis calculated risk ratios (RRs) and 95% confidence intervals (CIs) after assessing bias risk.</p><p><strong>Results: </strong>Six of the 323 screened studies met the inclusion criteria, encompassing 2169 patients: five studies included adult populations, and one included a pediatric population. Meta-analysis revealed no significant difference in 1-year overall survival between the anaerobic and the limited anaerobic coverage groups (RR: 1.01; 95% CI: 0.92-1.12). Acute GVHD incidence was significantly higher in the anaerobic coverage group than in the limited anaerobic coverage group (RR: 1.33; 95% CI: 1.17-1.51). GVHD-related mortality tended to be higher in the anaerobic coverage group than in the limited coverage group (RR: 1.65; 95% CI: 0.94-2.91). Of the six studies, three had a high risk of bias. Moderate heterogeneity was observed between citations regarding GVHD-related mortality (I<sup>2</sup> = 63%).</p><p><strong>Conclusion: </strong>Antibiotics with anaerobic coverage appear to increase acute GVHD incidence in patients who received an allogeneic HSCT compared to antibiotics with limited anaerobic coverage. However, the strength of this conclusion is limited by the quality of available evidence. Further well-designed research is necessary to clarify the impact of anaerobic antibiotic coverage on GVHD-related outcomes.</p>","PeriodicalId":23318,"journal":{"name":"Transplant Infectious Disease","volume":" ","pages":"e70049"},"PeriodicalIF":2.6000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12416444/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplant Infectious Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/tid.70049","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/29 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Broad-spectrum antibiotics are standard for febrile neutropenia (FN) in allogeneic hematopoietic stem cell transplantation (HSCT) but may disrupt gut microbiota, increasing the risk of graft-versus-host disease (GVHD). However, current evidence on the effects of anaerobic versus limited anaerobic antibiotic coverage on GVHD-related outcomes remains inconclusive.
Methods: We systematically searched for studies assessing overall survival, acute GVHD incidence, and GVHD-related mortality in patients with allogeneic HSCT receiving antibiotics with anaerobic versus limited anaerobic coverage. A random-effects meta-analysis calculated risk ratios (RRs) and 95% confidence intervals (CIs) after assessing bias risk.
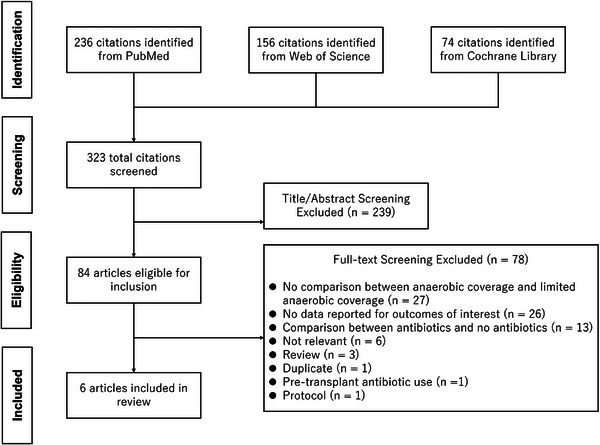
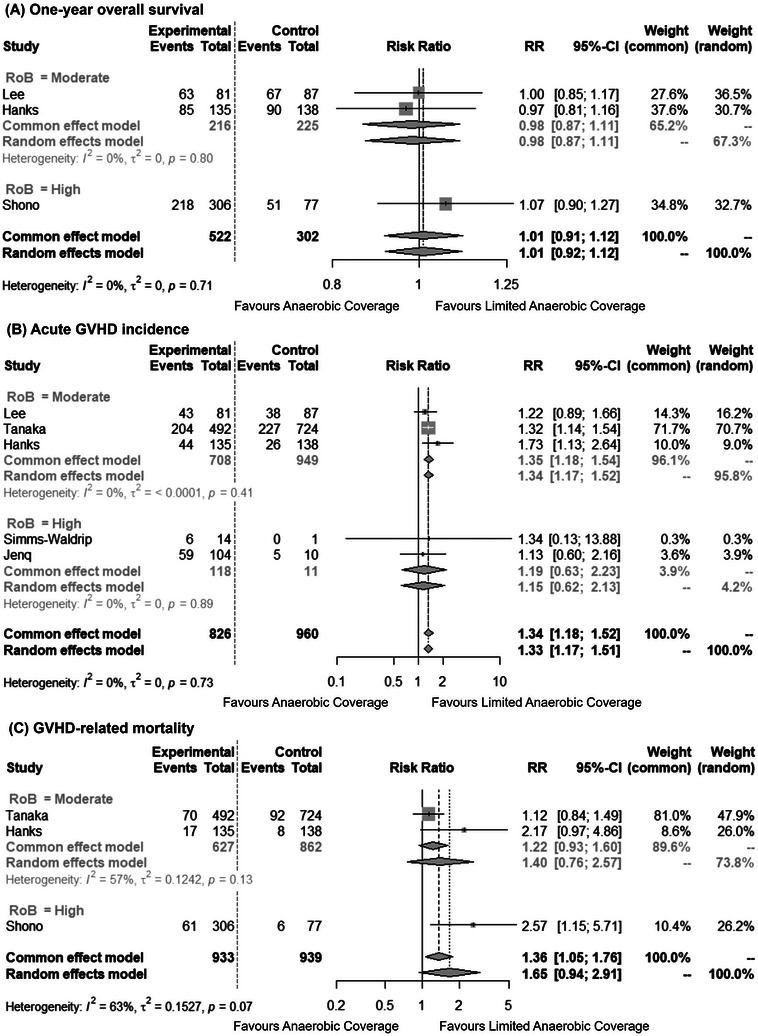
Results: Six of the 323 screened studies met the inclusion criteria, encompassing 2169 patients: five studies included adult populations, and one included a pediatric population. Meta-analysis revealed no significant difference in 1-year overall survival between the anaerobic and the limited anaerobic coverage groups (RR: 1.01; 95% CI: 0.92-1.12). Acute GVHD incidence was significantly higher in the anaerobic coverage group than in the limited anaerobic coverage group (RR: 1.33; 95% CI: 1.17-1.51). GVHD-related mortality tended to be higher in the anaerobic coverage group than in the limited coverage group (RR: 1.65; 95% CI: 0.94-2.91). Of the six studies, three had a high risk of bias. Moderate heterogeneity was observed between citations regarding GVHD-related mortality (I2 = 63%).
Conclusion: Antibiotics with anaerobic coverage appear to increase acute GVHD incidence in patients who received an allogeneic HSCT compared to antibiotics with limited anaerobic coverage. However, the strength of this conclusion is limited by the quality of available evidence. Further well-designed research is necessary to clarify the impact of anaerobic antibiotic coverage on GVHD-related outcomes.
期刊介绍:
Transplant Infectious Disease has been established as a forum for presenting the most current information on the prevention and treatment of infection complicating organ and bone marrow transplantation. The point of view of the journal is that infection and allograft rejection (or graft-versus-host disease) are closely intertwined, and that advances in one area will have immediate consequences on the other. The interaction of the transplant recipient with potential microbial invaders, the impact of immunosuppressive strategies on this interaction, and the effects of cytokines, growth factors, and chemokines liberated during the course of infections, rejection, or graft-versus-host disease are central to the interests and mission of this journal.
Transplant Infectious Disease is aimed at disseminating the latest information relevant to the infectious disease complications of transplantation to clinicians and scientists involved in bone marrow, kidney, liver, heart, lung, intestinal, and pancreatic transplantation. The infectious disease consequences and concerns regarding innovative transplant strategies, from novel immunosuppressive agents to xenotransplantation, are very much a concern of this journal. In addition, this journal feels a particular responsibility to inform primary care practitioners in the community, who increasingly are sharing the responsibility for the care of these patients, of the special considerations regarding the prevention and treatment of infection in transplant recipients. As exemplified by the international editorial board, articles are sought throughout the world that address both general issues and those of a more restricted geographic import.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


