{"title":"Endoscopic diagnosis of immunoglobulin G4-related sclerosing cholangitis.","authors":"Itaru Naitoh, Michihiro Yoshida, Takahiro Nakazawa","doi":"10.1111/den.15039","DOIUrl":null,"url":null,"abstract":"<p><p>Immunoglobulin G4 (IgG4)-related sclerosing cholangitis (IgG4-SC) is a distinct form of sclerosing cholangitis frequently associated with autoimmune pancreatitis and is recognized as a biliary manifestation of IgG4-related disease. Endoscopic retrograde cholangiopancreatography (ERCP) and endoscopic ultrasonography (EUS) are key diagnostic modalities for IgG4-SC. Cholangiocarcinoma and primary sclerosing cholangitis (PSC) are significant mimickers of IgG4-SC. ERCP is employed to evaluate narrowing of the bile duct, with cholangiograms of IgG4-SC classified into four types. This cholangiographic classification is crucial for differential diagnosis. Characteristic cholangiographic findings of IgG4-SC include diffuse or segmental strictures of the intrahepatic or extrahepatic bile ducts and intrahepatic strictures associated with autoimmune pancreatitis. ERCP is particularly useful for differentiating IgG4-SC from PSC because their cholangiographic features differ. EUS and intraductal ultrasonography (IDUS) are used to assess thickening of the bile duct wall. Characteristic IDUS findings in IgG4-SC include circular and symmetrical wall thickening, smooth outer and inner margins, and homogeneous internal echoes at stricture sites. Additionally, bile duct wall thickening at nonstricture sites is a typical IDUS feature of IgG4-SC. Bile duct biopsy is used to evaluate pathological findings, although its diagnostic yield for IgG4-SC is limited; its primary role is to exclude malignant biliary strictures. Duodenal papilla biopsy serves as a supplementary diagnostic tool for IgG4-SC. EUS and tissue acquisition also aid in diagnosing autoimmune pancreatitis as part of other organ involvement. Thus, endoscopic techniques play critical roles in the diagnosis of IgG4-SC.</p>","PeriodicalId":72813,"journal":{"name":"Digestive endoscopy : official journal of the Japan Gastroenterological Endoscopy Society","volume":" ","pages":"824-833"},"PeriodicalIF":4.7000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12333321/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive endoscopy : official journal of the Japan Gastroenterological Endoscopy Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1111/den.15039","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/21 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
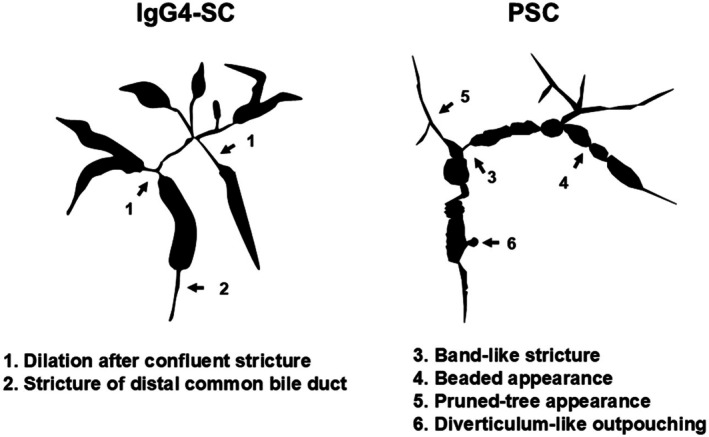
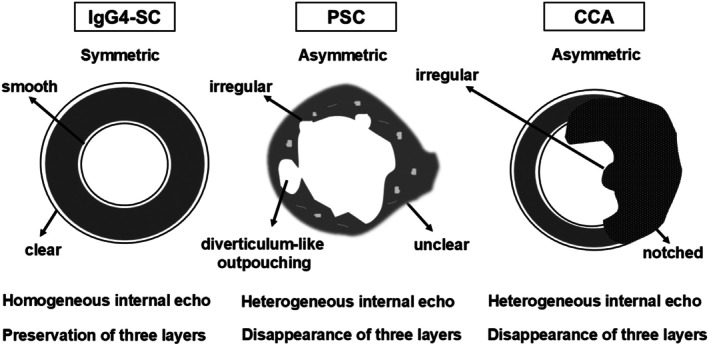
Immunoglobulin G4 (IgG4)-related sclerosing cholangitis (IgG4-SC) is a distinct form of sclerosing cholangitis frequently associated with autoimmune pancreatitis and is recognized as a biliary manifestation of IgG4-related disease. Endoscopic retrograde cholangiopancreatography (ERCP) and endoscopic ultrasonography (EUS) are key diagnostic modalities for IgG4-SC. Cholangiocarcinoma and primary sclerosing cholangitis (PSC) are significant mimickers of IgG4-SC. ERCP is employed to evaluate narrowing of the bile duct, with cholangiograms of IgG4-SC classified into four types. This cholangiographic classification is crucial for differential diagnosis. Characteristic cholangiographic findings of IgG4-SC include diffuse or segmental strictures of the intrahepatic or extrahepatic bile ducts and intrahepatic strictures associated with autoimmune pancreatitis. ERCP is particularly useful for differentiating IgG4-SC from PSC because their cholangiographic features differ. EUS and intraductal ultrasonography (IDUS) are used to assess thickening of the bile duct wall. Characteristic IDUS findings in IgG4-SC include circular and symmetrical wall thickening, smooth outer and inner margins, and homogeneous internal echoes at stricture sites. Additionally, bile duct wall thickening at nonstricture sites is a typical IDUS feature of IgG4-SC. Bile duct biopsy is used to evaluate pathological findings, although its diagnostic yield for IgG4-SC is limited; its primary role is to exclude malignant biliary strictures. Duodenal papilla biopsy serves as a supplementary diagnostic tool for IgG4-SC. EUS and tissue acquisition also aid in diagnosing autoimmune pancreatitis as part of other organ involvement. Thus, endoscopic techniques play critical roles in the diagnosis of IgG4-SC.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


