Mahmoud Tantawy, Marwan Saad, Sherif Hussien, Ghada Selim, Ahmed Tamara
{"title":"Predilation in Primary Percutaneous Coronary Intervention.","authors":"Mahmoud Tantawy, Marwan Saad, Sherif Hussien, Ghada Selim, Ahmed Tamara","doi":"10.15420/icr.2024.12","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In primary percutaneous coronary intervention (pPCI), balloon predilation is frequently carried out before stenting but there is a lack of data regarding optimal balloon size and the effect of balloon size on procedural and clinical outcomes.</p><p><strong>Aims: </strong>This study compares small balloon predilation (≤50% of proximal vessel diameter) with large balloon predilation (>50% of proximal vessel diameter) in pPCI.</p><p><strong>Methods: </strong>This multicentre prospective observational study included consecutive ST elevation MI (STEMI) patients undergoing pPCI at three tertiary centres in Egypt. Demographic, clinical and angiographic data were collected for all the patients. The primary outcome was the presence of no reflow at the conclusion of the procedure and secondary outcomes included procedural complications - no reflow, dissection, abrupt vessel closure, fluoroscopy time and procedural time - and clinical outcomes - in-hospital left ventricular ejection fraction (LVEF), cardiogenic shock, stent thrombosis, ventricular fibrillation, stroke, death, ST-segment resolution >50% 1 hour after PCI and LVEF at discharge.</p><p><strong>Results: </strong>A total of 384 pPCI procedures were included. The small balloon group (n=222) and the large balloon group (n=162) were comparable in terms of baseline characteristics. The large balloon group had a significantly higher incidence of no reflow (n=23 [14.2%] versus n=6 [2.7%], p<0.001), procedural complications: n=31 [19.4%] versus n=10 [4.5%], p<0.001) and contrast volume (190.4 ± 40.2 ml versus 177.4 ± 29.4 ml, p=0.0003) compared to the small balloon group. ST-segment resolution >50% after PCI was more frequent in the small balloon group (n=182 [81.98%] versus n=109 [67.28%], p<0.001).</p><p><strong>Conclusion: </strong>This study suggests that using a smaller balloon size for predilation in pPCI is associated with improved coronary flow, reduced procedural complications and better ST-segment resolution.</p>","PeriodicalId":38586,"journal":{"name":"Interventional Cardiology Review","volume":"20 ","pages":"e15"},"PeriodicalIF":2.8000,"publicationDate":"2025-04-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12060174/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interventional Cardiology Review","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15420/icr.2024.12","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"0","JCRName":"PHILOSOPHY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In primary percutaneous coronary intervention (pPCI), balloon predilation is frequently carried out before stenting but there is a lack of data regarding optimal balloon size and the effect of balloon size on procedural and clinical outcomes.
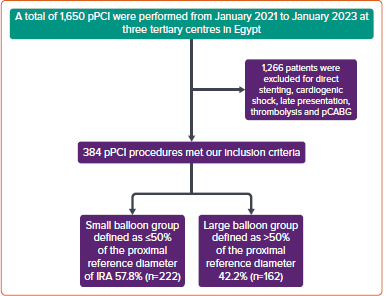
Aims: This study compares small balloon predilation (≤50% of proximal vessel diameter) with large balloon predilation (>50% of proximal vessel diameter) in pPCI.
Methods: This multicentre prospective observational study included consecutive ST elevation MI (STEMI) patients undergoing pPCI at three tertiary centres in Egypt. Demographic, clinical and angiographic data were collected for all the patients. The primary outcome was the presence of no reflow at the conclusion of the procedure and secondary outcomes included procedural complications - no reflow, dissection, abrupt vessel closure, fluoroscopy time and procedural time - and clinical outcomes - in-hospital left ventricular ejection fraction (LVEF), cardiogenic shock, stent thrombosis, ventricular fibrillation, stroke, death, ST-segment resolution >50% 1 hour after PCI and LVEF at discharge.
Results: A total of 384 pPCI procedures were included. The small balloon group (n=222) and the large balloon group (n=162) were comparable in terms of baseline characteristics. The large balloon group had a significantly higher incidence of no reflow (n=23 [14.2%] versus n=6 [2.7%], p<0.001), procedural complications: n=31 [19.4%] versus n=10 [4.5%], p<0.001) and contrast volume (190.4 ± 40.2 ml versus 177.4 ± 29.4 ml, p=0.0003) compared to the small balloon group. ST-segment resolution >50% after PCI was more frequent in the small balloon group (n=182 [81.98%] versus n=109 [67.28%], p<0.001).
Conclusion: This study suggests that using a smaller balloon size for predilation in pPCI is associated with improved coronary flow, reduced procedural complications and better ST-segment resolution.
背景:在初级经皮冠状动脉介入治疗(pPCI)中,球囊预扩张经常在支架置入前进行,但缺乏关于球囊最佳尺寸以及球囊尺寸对手术和临床结果影响的数据。目的:本研究比较小球囊预扩张(≤近端血管直径的50%)和大球囊预扩张(≤近端血管直径的50%)在pPCI中的应用。方法:这项多中心前瞻性观察研究包括在埃及三个三级中心接受pPCI的连续ST段抬高心肌梗死(STEMI)患者。收集所有患者的人口学、临床和血管造影资料。主要结果是手术结束时无再流,次要结果包括手术并发症-无再流、夹层、血管突然关闭、透视时间和手术时间-和临床结果-住院左室射血分数(LVEF)、心源性休克、支架血栓形成、心室颤动、中风、死亡、PCI术后1小时st段分辨率bbb50 %和出院时LVEF。结果:共纳入384例pPCI手术。小球囊组(n=222)和大球囊组(n=162)在基线特征方面具有可比性。大球囊组无血流再流发生率明显高于小球囊组(n=23 [14.2%] vs . n=6[2.7%]),小球囊组PCI术后p50%发生率更高(n=182 [81.98%] vs . n=109[67.28%])。结论:本研究表明,在pPCI中使用较小球囊进行预扩张可改善冠状动脉血流,减少手术并发症,改善st段分辨率。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


